What Are Zygomatic Implants?Complete Patient Guide
- Zygomatic implants are long titanium fixtures (30–52.5mm) anchored into the zygomatic (cheek) bone rather than the maxillary jawbone.
They are designed for patients with severe upper jaw bone loss who have been told they "don't have enough bone for implants" and want to avoid bone grafting.

How Zygomatic Implants Work
Conventional implants are 8–13mm long and require adequate jawbone volume. When the upper jaw has resorbed (shrunk) - common after years of tooth loss or denture wear - there isn't enough bone for conventional implants.
Zygomatic implants bypass the atrophied maxilla entirely. They're inserted through the jawbone and anchored into the zygomatic bone (cheekbone), which is dense, cortical, and doesn't resorb.
Questions about this procedure?
Who Needs Zygomatic Implants?
- Severe maxillary bone loss (Class V–VI atrophy)
- Failed previous bone grafting
- Long-term edentulism (10+ years without teeth)
- Patients who want to avoid 6–12 months of bone grafting and healing
- Patients previously told they're "not a candidate" for implants
Ready to discuss your options?
The Procedure
1. 3D CBCT imaging to assess zygomatic bone quality and plan trajectory
2. Surgery under IV sedation (or general anaesthesia)
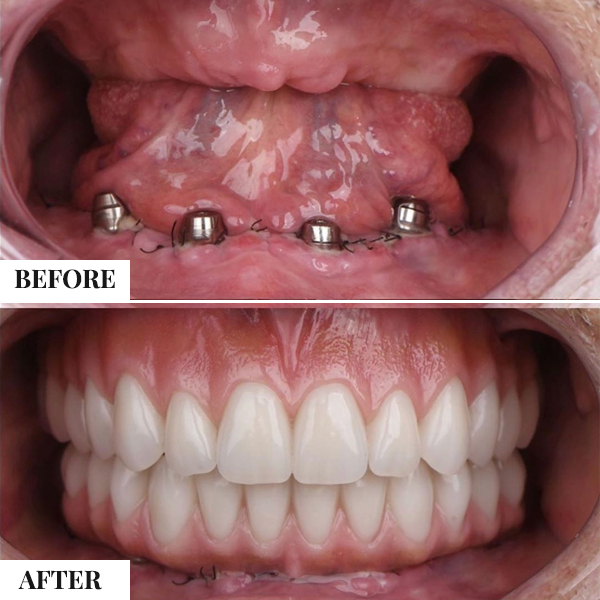
3. 2–4 zygomatic implants placed (+ conventional anterior implants if needed)
4. Immediate loading with provisional prosthesis (same-day teeth)
5. Definitive prosthesis after 4–6 months
Curious about costs and timelines?
Clinical Evidence
- 96.5% survival at 7+ years (Aparicio et al.)
- Immediate loading success: >95%
- Patient satisfaction: >90% (vs. removable prostheses)
- Reduced morbidity compared to extensive bone grafting
Want a personalised treatment plan?
Cost
| New Zealand (NZD) | Stunning Dentistry (NZD) | |
|---|---|---|
| Zygomatic (per arch) | on request | from on request |
| Quad zygomatic (both arches) | on request | from on request |
Questions about this procedure?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.