Smile Design in New Zealand, What Digital Planning Actually Does and What It Cannot
- Smile design as a clinical discipline emerged from the recognition that aesthetic dental changes affect facial balance in ways that are difficult to predict from dental study models alone.
A veneer that lengthens a central incisor by 1.5 mm changes the golden proportion relationship to the laterals and alters how the lip falls at rest.
Overview {#overview}
What is smile design?
> Smile design is a structured clinical process that maps the proportional, colour, and positional parameters of a patient's teeth and face before restorative treatment, translates those parameters into a digital plan, and uses that plan to guide the fabrication of veneers, crowns, or composite additions. It is a planning methodology, not a single procedure. The outcome is determined by the accuracy of the initial analysis, the quality of the restorations, and whether the patient's gingival and occlusal health supports the planned changes.
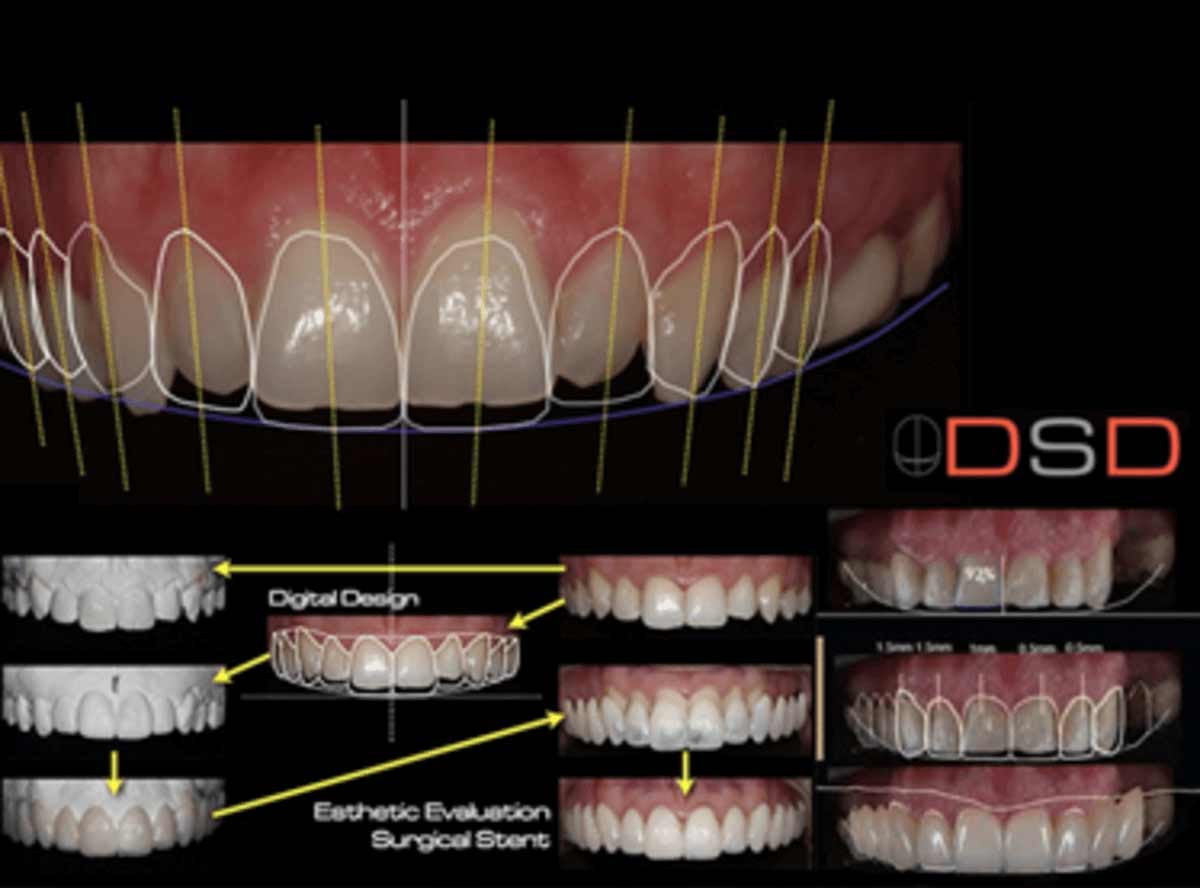
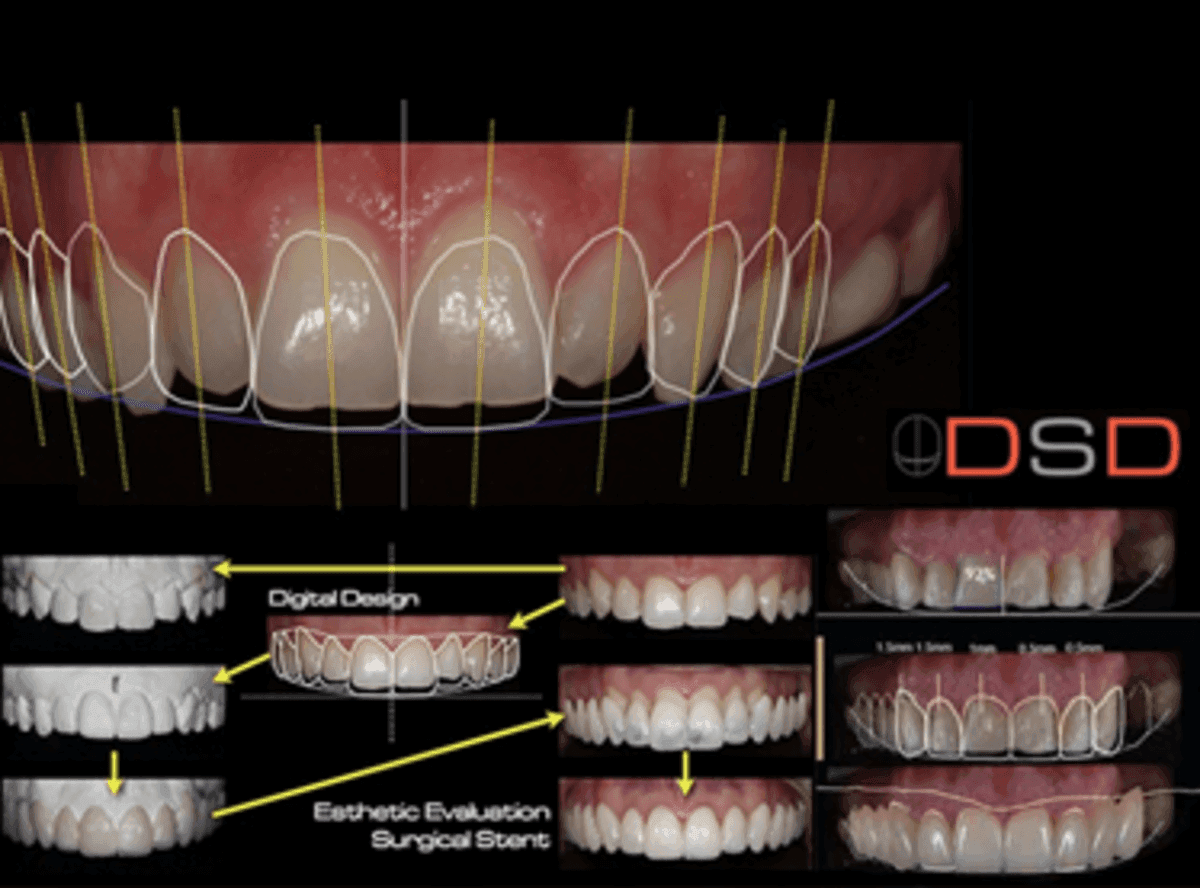
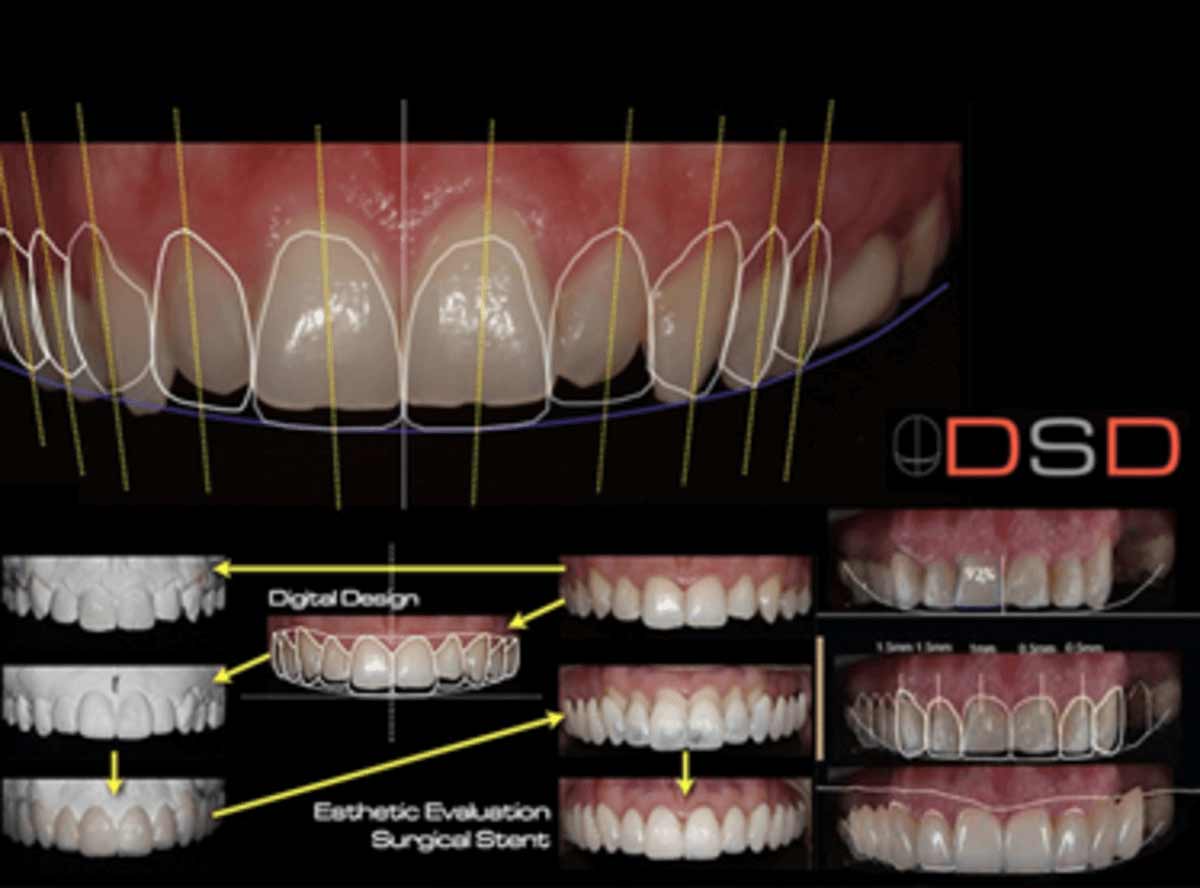
Smile design as a clinical discipline emerged from the recognition that aesthetic dental changes affect facial balance in ways that are difficult to predict from dental study models alone. A veneer that lengthens a central incisor by 1.5 mm changes the golden proportion relationship to the laterals and alters how the lip falls at rest. Digital Smile Design (DSD), most commonly the protocol developed by Christian Coachman, photographs the patient's face and teeth under standardised conditions, maps dental midline and facial midline, measures golden proportion ratios, incisal edge position relative to the lip, gingival zenith positions, and tooth length-to-width ratios. This mapping produces a digital template from which the planned restorations are designed before any tooth preparation begins.
At Stunning Dentistry, smile design cases begin with DSD photography and digital planning before any treatment is proposed. The digital plan is presented to the patient, adjusted to preference, and prototyped as a mock-up before any tooth preparation is agreed. Treatment proceeds only when the patient has seen and approved the three-dimensional prototype.
| Smile Design Step | Purpose | Reversible? |
|---|---|---|
| DSD photography and mapping | Capture baseline; measure proportions | Yes, no treatment |
| Digital plan and rendering | Preview outcome; adjust parameters | Yes, digital only |
| Mock-up (wax prototype) | Three-dimensional preview on patient's own teeth | Yes, no preparation |
| Patient approval | Confirm plan before irreversible treatment | Yes, last decision point |
| Tooth preparation (if required) | Reduce enamel for veneer or crown | No, irreversible |
| Temporaries | Trial period with long-term provisionals | Reversible within limits |
| Final restoration placement | Veneers, crowns, or composite bonding | No, irreversible |
Questions about this procedure?
What Digital Smile Design Measures {#what-dsd-measures}
What parameters does digital smile design assess?
> Digital Smile Design measures: facial midline vs dental midline alignment, incisal edge position relative to the relaxed upper lip (2–4 mm display at rest is the clinical norm), gingival zenith position (the highest point of the gum margin on each tooth), smile width (how many teeth show when smiling), incisal plane inclination, golden proportion ratios between tooth widths, and tooth length-to-width ratio (75–80% is considered aesthetic for upper centrals).
Facial and dental midlines: The dental midline (space between upper central incisors) ideally aligns with the facial midline (a line from the nose tip through the chin). A deviation of up to 2 mm is generally not perceptible to observers; deviations beyond 2–3 mm may be conspicuous. Correcting a midline discrepancy with veneers alone is only possible when the deviation is small, larger midline discrepancies may require orthodontic correction first.
At Stunning Dentistry, DSD is performed by our restorative team using standardised retracted and non-retracted smile photography. The digital plan is overlaid on the patient's photograph and reviewed with the patient at the consultation appointment before any treatment decisions are made.
Ready to discuss your options?
The Four Pathways: Which One Applies to You {#four-pathways}
Smile design cases fall into four primary clinical pathways based on what changes are needed and what the underlying anatomy supports:
| Pathway | What Changes | Primary Restorations | Tooth Preparation |
|---|---|---|---|
| 1. Composite addition | Shape, minor length, small gaps | Composite bonding | None (additive only) |
| 2. Veneer restoration | Colour, shape, significant length, surface | Porcelain veneers | Minimal enamel reduction (0.3–0.7 mm) |
| 3. Full coverage | Broken, heavily restored, or crown-height-space cases | All-ceramic crowns | Full preparation (1.5–2.5 mm reduction) |
| 4. Complex multi-system | Midline correction + gingival recontouring + veneers | DSD-guided multimodal | Variable by component |
Curious about costs and timelines?

Porcelain Veneers, Clinical Reality {#porcelain-veneers}
What are porcelain veneers?
8 mm) bonded to the buccal (front) surface of the teeth to change colour, shape, or surface texture. 7 mm of enamel reduction to create space for the veneer and a resin cement bond layer. Once prepared, the tooth requires permanent veneer coverage for its lifetime.
Porcelain veneers are fabricated by a dental ceramist from feldspar porcelain (most translucent; most natural-looking; lower strength) or lithium disilicate ceramic (IPS e.max, higher strength; excellent translucency; used for most cases). The veneer is bonded to the prepared enamel surface using resin cement and a light-curing protocol that creates a chemical-mechanical bond. The bond strength is enamel-dependent: veneers bonded predominantly to enamel have higher long-term survival than veneers bonded to dentine (which is softer and more porous).
At Stunning Dentistry, porcelain veneers are fabricated using IPS e.max lithium disilicate by accredited ceramists. All veneer cases include a wax-up mock-up evaluated at a preparation appointment before any enamel is removed. Patients who have not had a periodontal and occlusal assessment elsewhere will have one completed before treatment proceeds.
| Ceramic Material | Strength | Translucency | Preparation Required | Best For |
|---|---|---|---|---|
| Feldspathic porcelain | Moderate | Highest | 0.3–0.5 mm | Minimal prep; high-aesthetic anterior |
| Lithium disilicate (e.max) | High | High | 0.4–0.7 mm | Most veneer cases; durable |
| Zirconia (monolithic) | Very high | Lower | 0.5–0.8 mm | Posterior cases; parafunctional patients |
Want a personalised treatment plan?

Composite Bonding, Clinical Reality {#composite-bonding}
Composite bonding uses direct resin composite, the same material used for white fillings, applied freehand or through a putty-index template to the front surface of the teeth to change shape, close small gaps (diastemas), or mask surface discolouration. Unlike porcelain veneers, composite bonding requires no tooth preparation when used additively and can, in principle, be removed or revised.
At Stunning Dentistry, composite bonding cases are assessed at DSD consultation for appropriateness. Minor diastema closure, edge chipping repair, and small shape corrections are well-suited to composite. Full-arch aesthetic restorations intended to last more than 5 years are typically planned as porcelain veneer cases.
Questions about this procedure?
Crowns in Smile Design {#crowns-in-smile-design}
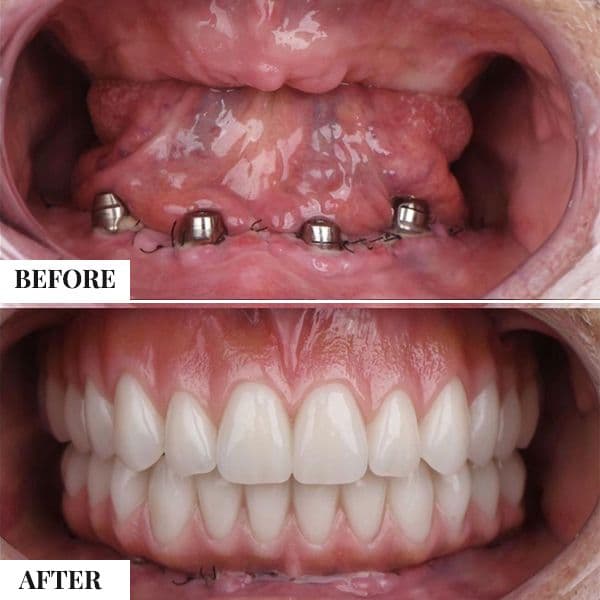
Crowns are used in smile design cases where teeth are too structurally compromised for veneer coverage (large existing fillings, heavily broken teeth, short clinical crowns requiring full coverage for occlusal adjustment), or where the restorative plan includes a full arch change that extends to the posterior teeth. In these cases, the DSD-guided ceramic crown allows colour and shape to be precisely designed from the digital template.
Crown preparation is more extensive than veneer preparation, typically 1.5–2.5 mm of circumferential reduction, and commits the tooth to permanent crown coverage. The decision to use a crown versus a veneer depends on the existing tooth structure available and the functional requirements of the restoration.
Ready to discuss your options?
The Mock-Up Step, Why It Matters {#mock-up}
The mock-up, a physical three-dimensional prototype of the planned restorations placed temporarily on the patient's unprepared teeth, is the most important patient safety step in smile design. The mock-up may be fabricated as a wax-up on a stone model and photographed against the patient's DSD template, or it may be realised as a direct provisional composite prototype applied to the unprepared teeth at a try-in appointment. The patient wears the provisional prototype and evaluates: tooth length, smile width, phonetics (whether certain sounds are affected), lip profile, and general aesthetic response.
At Stunning Dentistry, no veneer preparation proceeds without a prior mock-up. The mock-up approval is documented and signed, and the ceramist receives the DSD-guided specifications derived from the approved prototype before fabrication begins.
Curious about costs and timelines?
Occlusion and Smile Design, The Safety Gate {#occlusion-safety}
Occlusion, the way the upper and lower teeth meet in function, lateral movement, and excursive contact, is the primary clinical risk in smile design. Porcelain veneers on the anterior teeth are loaded in lateral excursion when the upper anterior teeth slide against the lower anterior teeth during jaw movements (canine guidance or group function). If this load exceeds the ceramic fracture threshold or disrupts the resin-ceramic bond, veneers chip or debond.
Occlusal analysis also determines whether anterior veneers can be made in their ideal position without interfering with the bite, a problem called insufficient crown height space. If the upper and lower anterior teeth meet with very little clearance in the planned veneer position, the veneer will be in occlusal contact and will chip. This may require either a reduced veneer thickness (compromising aesthetics) or anterior bite opening (raising the vertical dimension to create space), a more complex and expensive intervention.
Want a personalised treatment plan?
What Smile Design Cannot Change {#limitations}
Understanding the boundaries of what smile design can and cannot achieve prevents unrealistic expectations:
| Parameter | Can Smile Design Change It? | Notes |
|---|---|---|
| Tooth colour | Yes | Veneers or bleaching; within material limits |
| Tooth shape | Yes | Addition or reduction-based |
| Tooth length | Yes (to a point) | Limited by gum position; gingival recontouring may be required |
| Tooth alignment | Partially | Minor rotation or spacing only; significant misalignment requires orthodontics |
| Midline position | Partially | Up to 2 mm optical correction; more requires orthodontics |
| Gum levels | No (directly) | Gingival recontouring (gingivoplasty) is a separate procedure |
| Jaw size or profile | No | Jaw surgery (orthognathic) is required |
| Lip shape or fullness | No | Facial/aesthetic medicine; outside dental scope |
| Deep skeletal bite | No (directly) | Orthodontic/surgical correction first; veneers are then placed on corrected anatomy |
Questions about this procedure?
Risk Transparency {#risk-transparency}
Veneer fracture is the most commonly reported complication of porcelain veneer restorations. Reported fracture rates at 5–10 years range from 4–12% depending on material, occlusal loading, and patient parafunctional habits. Lithium disilicate (e.max) veneers have lower fracture rates than feldspathic porcelain at equivalent preparation thicknesses. Bruxism without an occlusal splint increases fracture risk by approximately 2–3 times.
Sensitivity after veneer preparation is common (affecting up to 40% of teeth in the first week), typically resolves within 2–4 weeks, and is related to the dentinal tubules exposed during enamel reduction. Persistent sensitivity beyond 4–6 weeks warrants assessment for pulpal involvement.
Ready to discuss your options?

Cost in NZD {#cost-in-nzd}
Total saving estimate, 8-tooth upper veneer case: NZD 14,400–22,400 (NZ) vs NZD 5,440–8,800 (Stunning Dentistry + travel). Net saving after NZD 1,800–2,400 return flight from Auckland or Christchurch to Hyderabad: approximately NZD 6,800–13,400.
| Procedure | NZ Private Cost (NZD) | Stunning Dentistry (NZD) |
|---|---|---|
| Digital Smile Design consultation and planning | $400–$900 | Included in treatment fee |
| Composite bonding per tooth | $400–$800 | $180–$350 |
| Composite bonding, 4-tooth anterior (upper) | $1,600–$3,200 | $720–$1,400 |
| Composite bonding, full 8-tooth upper arch | $3,200–$6,400 | $1,440–$2,800 |
| Porcelain veneer (e.max), per tooth | $1,800–$2,800 | $680–$1,100 |
| Porcelain veneers, 4 upper anterior | $7,200–$11,200 | $2,720–$4,400 |
| Porcelain veneers, full 8-tooth upper arch | $14,400–$22,400 | $5,440–$8,800 |
| Porcelain veneers, 16-tooth full arch (upper + lower 8) | $28,800–$44,800 | $10,880–$17,600 |
| All-ceramic crown (e.max), per tooth | $1,600–$2,600 | $580–$950 |
| Gingival recontouring (per arch, laser) | $800–$1,500 | $380–$680 |
| Wax-up mock-up (per arch) | $400–$800 | Included |
Curious about costs and timelines?
Myth vs Reality {#myth-vs-reality}
** "Veneers are permanent and cannot be reversed."
** Veneer placement requires enamel reduction, which is irreversible, the tooth permanently requires veneer or crown coverage thereafter. However, veneers themselves can be replaced when they wear or fracture. The permanent commitment is to veneer coverage of the tooth, not to the specific veneer.
** "Composite bonding is just as good as veneers but cheaper."
** Composite and porcelain serve different clinical indications. Composite stains, wears faster, and lacks the optical qualities of ceramic. It is appropriate for limited additive corrections and emergency repairs. For full-arch aesthetic change intended to last 10+ years, porcelain veneers are the clinical standard.
** "Smile design can fix any smile."
** Smile design is a planning methodology bounded by biology. Significant midline discrepancy, jaw skeletal asymmetry, deep skeletal bite, and severe gingival irregularity require orthodontic, surgical, or periodontal intervention before restorative smile design proceeds. DSD identifies these boundaries at the planning stage, before treatment is committed.
** "Hollywood smiles look obviously fake."
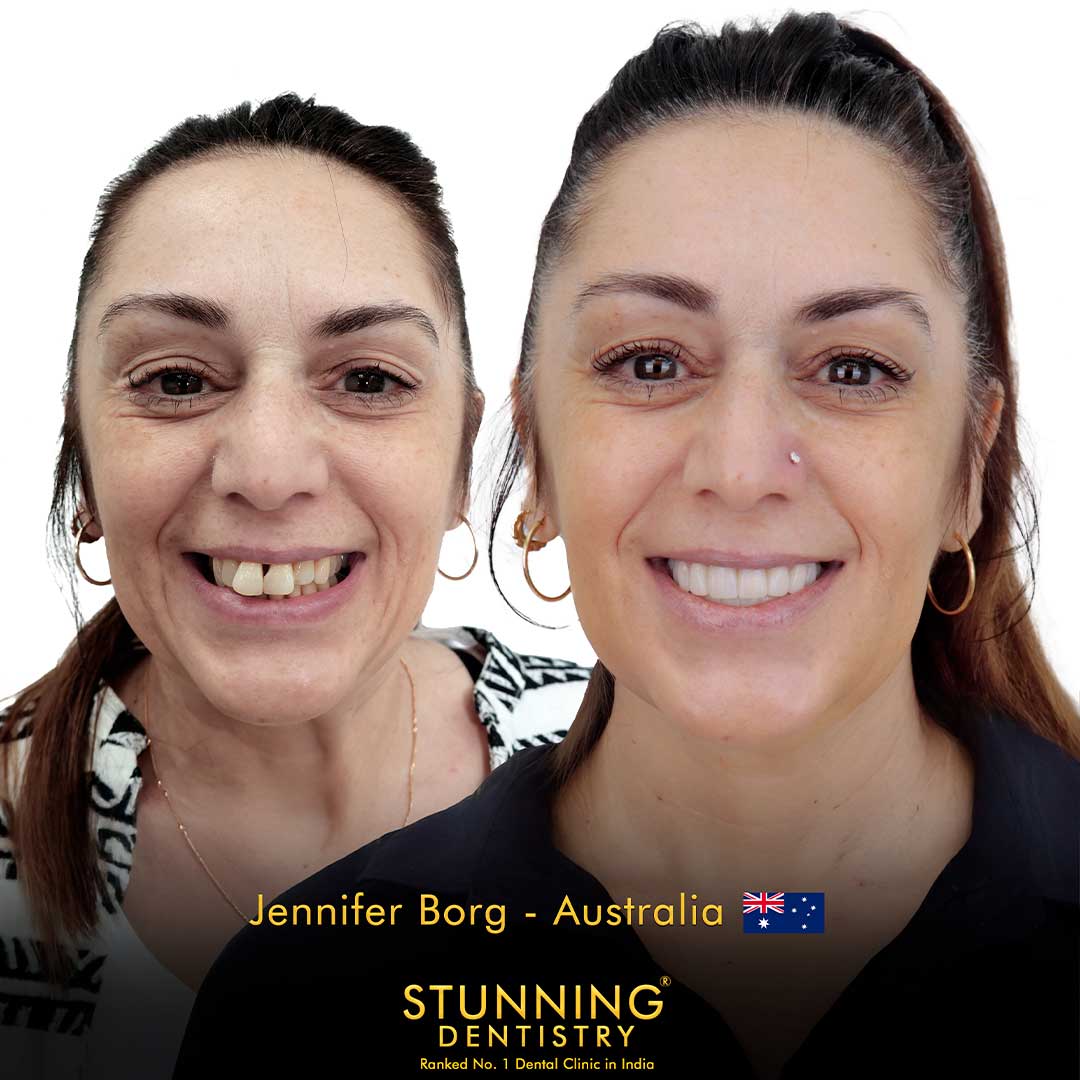
** Appropriate smile design, guided by facial proportion analysis, individual tooth-length-to-width ratios, and material selection matched to the patient's remaining tooth shade, produces restorations that are indistinguishable from natural teeth to observers. Conspicuous results are typically produced by over-whitened or over-sized ceramics made without DSD measurement.
Want a personalised treatment plan?

For Kiwi Patients: What to Bring to Consultation {#kiwi-consultation}
Smile design consultations are enhanced by the information Kiwi patients can bring from New Zealand before travel. Useful to bring or send in advance: current photographs of your smile (natural and posed), records of any prior dental work on the relevant teeth (most recent periapical X-rays, any existing crown or veneer information), information about grinding habits or prior splint use, and the specific aesthetic concerns you want to address.
Many patients find it useful to collect 3–5 reference images of smiles they find attractive, not to replicate them, but to help the restorative team understand the aesthetic direction preferred (longer vs shorter teeth, brighter vs more natural colour, wider vs narrower smile arc). These images are used as inspiration during the DSD session, not as templates.
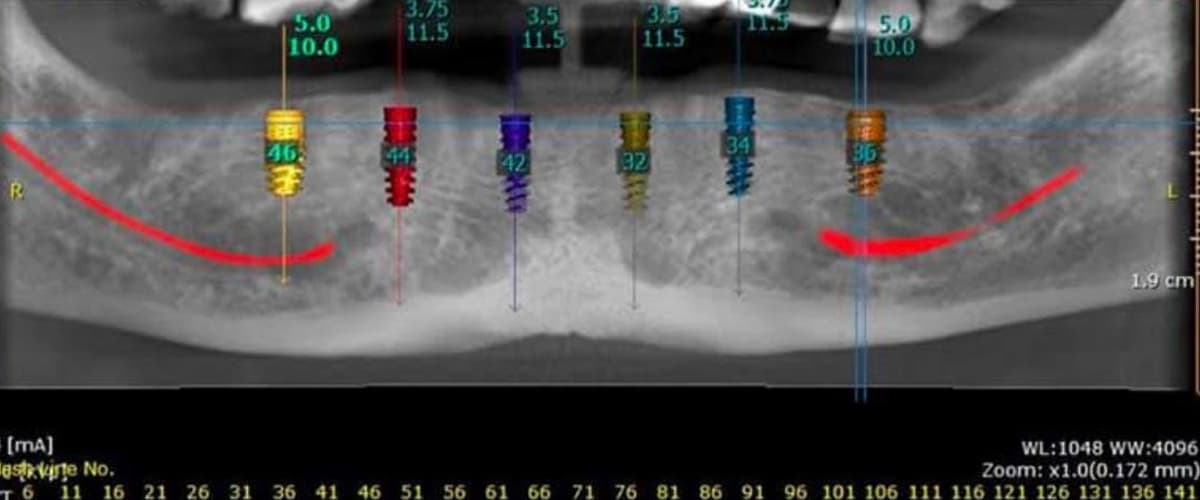
For Kiwi patients from Auckland, Wellington, Christchurch, Dunedin, Hamilton, Tauranga, or Queenstown planning a combined implant and smile design trip, the smile design component is sequenced after the implant restorations are complete, the aesthetic proportions of the final smile are determined after the implant-supported teeth have been placed and are stable. Ella Watson, Stunning Dentistry's Australasian patient liaison, coordinates this sequencing during the treatment planning phase.
Questions about this procedure?
People Also Ask {#people-also-ask}
What is the difference between a smile makeover and smile design?
DSD photography and planning is included in the treatment consultation fee. Wax-up mock-ups are included in the veneer treatment fee. Individual component costs (per veneer, per crown) are quoted from the treatment plan.
Ready to discuss your options?
Ask Your Doctor {#ask-your-doctor}
- What specific proportion issues does the DSD analysis show for my case?
- Which pathway applies to my teeth, composite, veneers, crowns, or a combination?
- What material will be used for my veneers, feldspathic or lithium disilicate?
- Will I need gingival recontouring before veneer placement?
- What does the occlusal assessment show, is my bite pattern a risk for veneers?
- Will I have a wax-up mock-up before any teeth are prepared?
- Do I have bruxism, and if so, what is the management plan before veneers?
- How much enamel will be removed at preparation, and is any of my case touching dentine?
Curious about costs and timelines?
Want a personalised treatment plan?
Book a Consultation {#book-a-consultation}
If you would like to discuss smile design options with reference to your specific tooth and facial anatomy:
*Protocols aligned with DCNZ cosmetic and restorative dentistry standards and DSD accreditation framework.*
Questions about this procedure?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Can I have veneers if I have a deep overbite?
A deep overbite (where the upper front teeth excessively cover the lower front teeth at rest) creates heavy contact on the palatal surface of the upper incisors during lateral movement. Veneers placed without addressing this contact will be in heavy functional loading and have a higher fracture risk. Management options include: a thin high-strength material (zirconia-reinforced composite or zirconia), orthodontic correction of the overbite before veneers, or anterior bite opening (raising the vertical dimension) as part of the smile design plan. None of these are simple; the correct approach depends on the degree of overbite and the patient's other clinical factors.
Can smile design fix a gummy smile?
A gummy smile, excessive gingival display when smiling, may have four possible causes: short clinical crowns, excessive gingival tissue covering normal-length teeth, vertical maxillary excess (jaw bone too long), or hypermobile upper lip. The treatment depends on the cause. Short crowns are addressed by crown lengthening; excessive gingival tissue by gingivoplasty; vertical maxillary excess by jaw surgery. DSD identifies which cause is present before treatment is offered.
Can I bleach my teeth before veneers?
Bleaching before veneer placement is standard practice when natural teeth will remain visible alongside the veneered teeth. The veneers are shade-matched to the post-bleaching tooth colour, not the pre-bleaching colour. Bleaching is typically completed 2–3 weeks before the veneer shade-matching appointment, as tooth colour continues to shift for 1–2 weeks after bleaching ends. Veneers cannot be bleached after placement; if natural teeth are bleached later, they may become lighter than the veneer shade.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.