All-on-4 Dental Implants for New Zealand Patients, The Maló Protocol, Honestly Explained
- What All-on-4 Actually Is, The Maló Protocol
What Is All-on-4 Dental Implants for New Zealand Patients?
What is All-on-4 for New Zealand patients?
> All-on-4 is a full-arch fixed prosthesis supported by four implants, using Dr Paulo Maló's tilting protocol to bypass the need for bone grafts in most cases. For New Zealand patients, the same treatment costs NZD 14,500–19,800 per arch at Stunning Dentistry versus NZD 38,000–52,000 at a private New Zealand specialist, saving NZD 20,000–35,000 per arch even after return flights from Auckland, Wellington, or Christchurch.
All-on-4 is a full-arch fixed prosthesis supported by four implants, the most studied full-arch implant protocol in the world. Developed by Dr Paulo Maló in Lisbon in the late 1990s, with five-year cumulative survival around 96% and 10-year survival around 94% across large published cohorts (Maló et al., 2011, 2014, 2019; Testori 2017; Cochrane review 2022), All-on-4 converts the edentulous or near-edentulous arch to a fixed 12–14-tooth bridge on four implants in a single surgical session.
For patients reading from Aotearoa New Zealand: the clinical protocol, material standards, and implant systems used here, Straumann SLActive, Nobel Biocare NobelActive, are identical to those used by DCNZ-registered implantologists in Auckland, Wellington, and Christchurch. What changes is the cost (55–70% lower, driven by Indian labour and facility differentials), the specialist bench depth on every case, and the in-house digital infrastructure. The 35 Ncm torque gate, the PMMA provisional, and the 4-6-month osseointegration period are the same in every country.
At Stunning Dentistry, every All-on-4 case is governed by the same Maló protocol used in the published 924-case cohort cited above: surgical guide from CBCT-derived virtual plan, torque verified fixture-by-fixture at surgery, provisional fitted only where the 35 Ncm threshold is met. 86.5% of patients leave with same-day fixed provisional teeth. 13.5% leave with healing abutments and return at month 4 for the fixed provisional. The fee is the same in both scenarios, the difference is trip sequencing, not clinical compromise.
| All-on-4 Cost | NZ Private Specialist (NZD) | Stunning Dentistry (NZD) | Net Saving |
|---|---|---|---|
| Single arch, all-inclusive | 38,000–52,000 | 14,500–19,800 | ~23,500–32,200 |
| Both arches, all-inclusive | 68,000–96,000 | 27,500–37,000 | ~40,500–59,000 |
| CBCT + digital planning + guide | 2,800–4,500 | Included | , |
| IV sedation + anaesthetist | 1,200–2,200 | Included | , |
| Milled PMMA provisional | 4,500–7,500 | Included | , |
| Monolithic zirconia definitive | 12,000–18,000 | Included | , |
| Return flights AKL/WLG/CHC → HYD | , | 1,300–2,200 (economy) | , |
| 10 nights hotel (4-star) | , | 700–1,200 | , |
| **Total NZD out-of-pocket (both arches, incl. travel)** | **68,000–96,000** | **~29,500–40,400** | **~28,000–55,600** |
Questions about this procedure?
What All-on-4 Actually Is, The Maló Protocol
What is the Maló Protocol for All-on-4?
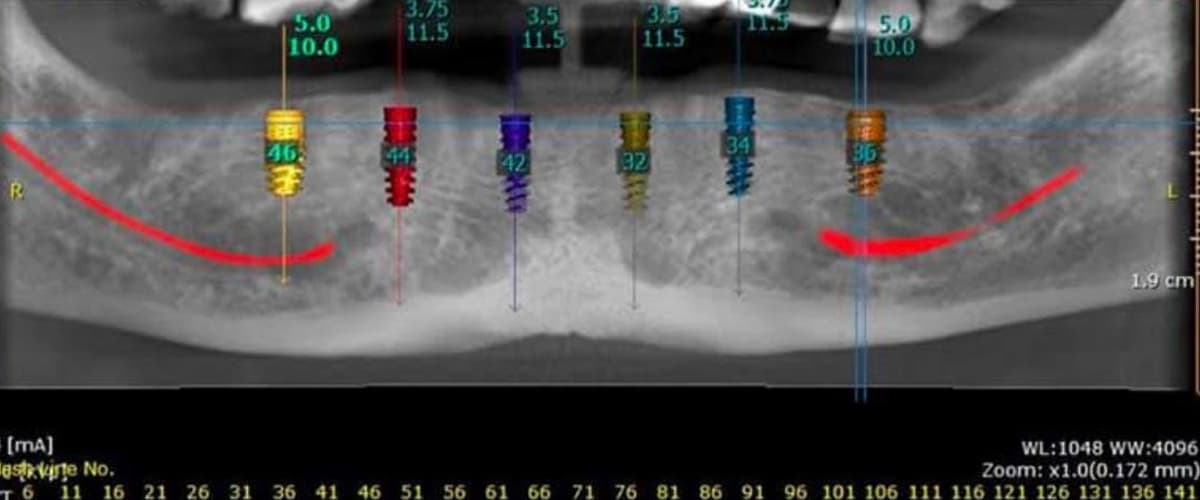
> Dr Paulo Maló's central insight was that the posterior maxillary sinus and mandibular canal do not need to be avoided by bone grafting, they can be avoided by tilting the two posterior implants 30–45° anteriorly. A tilted posterior fixture exits the bone anterior to the sinus or canal, lands in denser native bone, and supports a cantilevered prosthesis with improved anteroposterior spread. This eliminates the need for sinus lifts or posterior bone grafts in approximately 86–88% of cases, reducing total treatment time from 9–12 months (grafted approach) to 4–6 months.
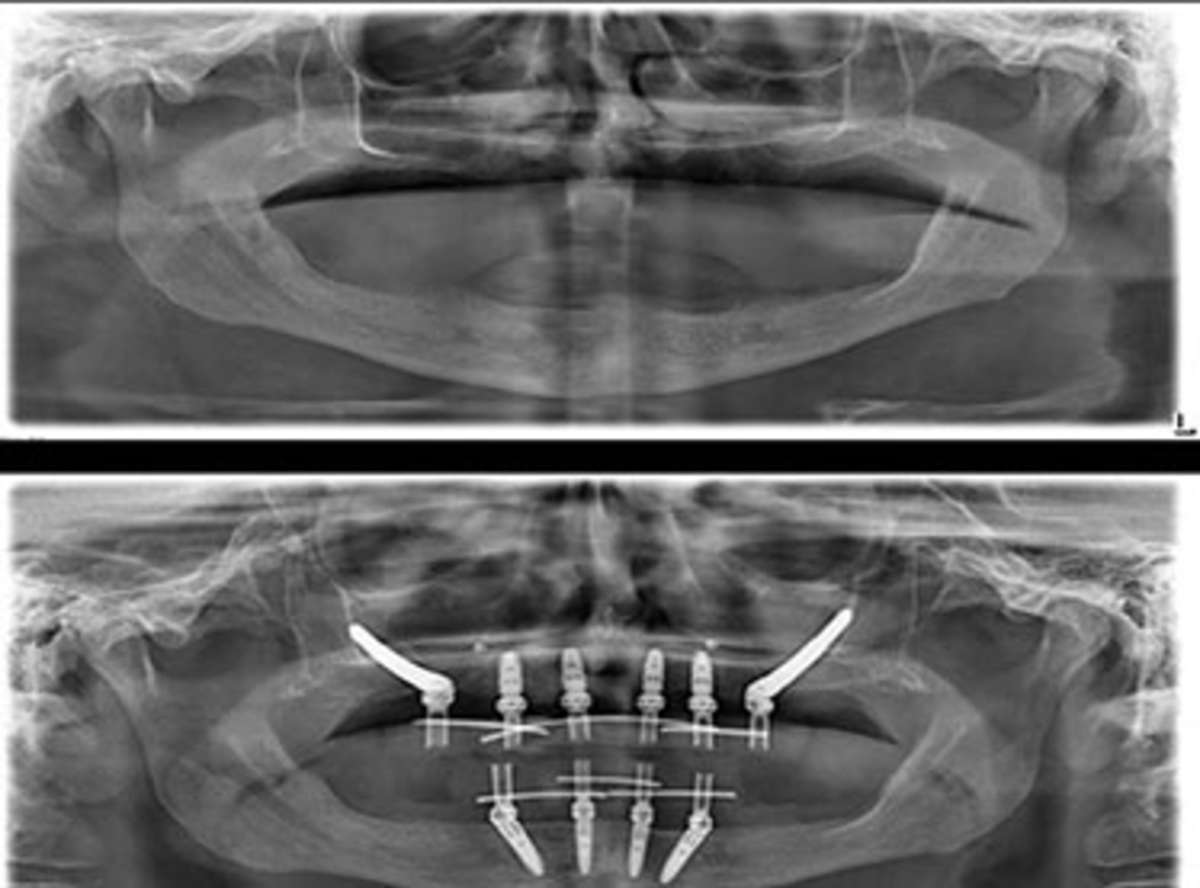
All-on-4 converts the edentulous or near-edentulous arch to a fixed 12–14-tooth bridge by distributing load across four strategically placed implants. Two anterior implants are placed vertically at the lateral incisor or canine position. Two posterior implants are tilted 30–45° distally, landing at the second premolar or first molar position through native bone, anterior to the sinus floor in the maxilla, anterior to the inferior alveolar canal in the mandible.
Why Tilting Works
- Longer implant in denser cortical bone (versus short vertical implant in spongy posterior bone)
- Greater A-P spread reduces cantilever moment on the prosthesis
- Avoids sinus floor and inferior alveolar canal without grafting
- Eliminates the 6-month graft-healing window in most cases
| Implant | Position | Orientation | Purpose |
|---|---|---|---|
| Anterior left | Lateral incisor or canine | Vertical (0°) | Anterior platform, aesthetic zone |
| Anterior right | Lateral incisor or canine | Vertical (0°) | Anterior platform, aesthetic zone |
| Posterior left | 2nd premolar / 1st molar | Tilted 30–45° distally | Extends A-P spread; avoids sinus/IAN |
| Posterior right | 2nd premolar / 1st molar | Tilted 30–45° distally | Extends A-P spread; avoids sinus/IAN |
Ready to discuss your options?
Who Is a Candidate, and Who Isn't
Who is a candidate for All-on-4?
> Strong candidates: failing full arch, adequate anterior bone height (typically 10+ mm), moderate posterior atrophy, non-smoker or willing to abstain perioperatively, physiologically fit for IV sedation. Borderline cases, documented bruxism, natural opposing dentition, insistence on molar-to-molar span, are better served by All-on-6. Severe posterior maxillary atrophy (ZAGA III–IV, <4 mm residual bone) points to zygomatic implants. 5%), recent head/neck radiotherapy, active heavy smoking without abstinence willingness.
All-on-4 candidacy is determined by bone volume, bite force profile, systemic health, and the ability to commit to the osseointegration period. The diagnosis precedes the plan, no credible implantologist commits to All-on-4 before reviewing the CBCT.
At Stunning Dentistry, New Zealand patients arriving with an All-on-4 quote from a NZ dentist are screened against this candidacy framework at the remote CBCT review before their first India visit. In 6% of cases, the CBCT confirms zygomatic is the safer plan. In 9%, All-on-6 is more appropriate for the bite-force profile. In 3%, a less extensive intervention is adequate. The remaining 82% proceed as planned.
| Profile | Recommendation | Clinical Reason |
|---|---|---|
| Failing full arch, moderate posterior atrophy, non-smoker | All-on-4 | Tilted posterior fixtures bypass sinus/IAN without grafting |
| Documented bruxism, natural opposing arch | All-on-6 | Greater load distribution; reduced cantilever stress |
| Severe posterior maxillary atrophy (ZAGA III–IV) | Zygomatic implants | Insufficient maxillary bone for any standard implant |
| HbA1c >8.5%, uncontrolled diabetes | Defer until systemic control | Osseointegration failure rate doubles above this threshold |
| Active smoker, unwilling to abstain | High-risk discussion; consider delay | Implant survival rate drops 2× in active smokers |
| Recent head/neck radiotherapy (<2 years) | Contraindicated | Radiation-damaged bone cannot support osseointegration reliably |
Curious about costs and timelines?

When NOT to Choose All-on-4
When is All-on-4 not the right choice?
> All-on-4 is not appropriate for: severe posterior maxillary atrophy (zygomatic protocol is safer); documented uncontrolled bruxism with natural opposing dentition (All-on-6 distributes load better); salvageable dentitions where a hybrid FMR preserves viable teeth; and patients who cannot commit to the 4-6 month osseointegration period between provisional and definitive.
All-on-4 is not universally applicable to all failing full-arch presentations. The most common over-indication is applying All-on-4 to a dentition that could be partially salvaged, where a hybrid FMR would preserve four or five viable teeth and reduce the overall treatment scope and cost. The decision to extract everything and start with four implants is correct for a terminal dentition; it is an over-treatment for a partially salvageable one.
At Stunning Dentistry, patients who cannot commit to the second visit within the required window are counselled before treatment begins, not during the provisional phase. If the two-visit commitment cannot be made, the treatment does not begin. Provisional-phase overextension is the single most preventable cause of All-on-4 complication, and it is prevented by honest pre-treatment planning, not surgical skill.
Want a personalised treatment plan?

Step-by-Step: The 10-Day Trip
What happens during the 10-day All-on-4 trip from New Zealand?
> Day 1: arrive Hyderabad, hotel check-in. Day 2: full CBCT, intraoral scans, photographs, bloods, anaesthetist consultation. Day 3: virtual implant plan, surgical guide printed. Day 4: surgery under IV sedation, extractions, ridge modification, four implants placed through guide, torque verified per fixture, PMMA provisional fitted where ≥35 Ncm met (~4 hours total chair time). Days 5–7: post-op reviews, swelling management, diet guidance. Day 8: photographs, comprehensive review. Days 9–10: fly home. Month 4–6: return visit (5 nights) for definitive monolithic zirconia prosthesis.
The 10-day structure is not arbitrary. Surgery on Day 4 is deliberate: three days of acclimatisation, jet-lag recovery, and diagnostic workup before any irreversible step. Five days of clinical monitoring after surgery before flying. The provisional phase runs for 4–6 months in New Zealand, concurrent with osseointegration, before the second trip for the definitive.
Pre-Travel (4–8 weeks before Visit 1): Remote consultation with Ella Watson (Australasian patient liaison). Medical questionnaire. Photograph and CBCT review if available. Financial paperwork in NZD. Flight booking: Singapore Airlines, Air NZ/Singapore codeshare, Qantas via Sydney, Emirates via Dubai, or Qatar via Doha from Auckland (AKL), Wellington (WLG), Christchurch (CHC), or Queenstown (ZQN) to Hyderabad (HYD).
Day 1: Arrive HYD. Airport transfer to hotel (Taj Krishna, Park Hyatt, ITC Kohenur, Novotel HITEC City, or similar). Rest.
Day 2: Full diagnostic workup, Carestream CS 9600 CBCT, Medit i700 intraoral scan, high-resolution photographs, blood panel, anaesthetist consultation.
Day 3: Virtual implant plan built in coDiagnostiX or Nobel Clinician. Surgical guide 3D-printed and verified. Patient reviews and approves the planned implant positions.
Day 4: Surgery under IV sedation with nitrous oxide inhalation supplementation available. Extractions (if needed). Ridge modification (where indicated). Four implants placed through printed guide. Torque verified fixture-by-fixture and documented. Immediate milled PMMA provisional fitted where all fixtures ≥35 Ncm. Total chair time approximately 4 hours.
Days 5–7: Post-op reviews: swelling management, bite adjustment, oral hygiene reinforcement, soft-diet counselling. Rest days.
Day 8: Photographs, comprehensive clinical check, discharge planning.
Days 9–10: Final review, written discharge plan, fly home. Soft diet 12 weeks. Bi-weekly Zoom check-ins with assigned prosthodontist.
Month 4–6 (Visit 2, 5 nights): Provisional phase reviewed. Final digital impressions. Monolithic zirconia definitive fabricated in-house. Fitted and adjusted. Occlusal equilibration. Night-guard provided. Warranty documentation issued.
At Stunning Dentistry, the itinerary above is handed to every New Zealand patient as a printed document before they book flights, not after. The logic behind Day 4 surgery, Day 8 final review, and the minimum-5-days-post-op departure rule is explained in writing. Nothing about the India visit is improvised on arrival.
| Day | Activity |
|---|---|
| Day 1 | Arrive Hyderabad. Airport transfer. Hotel check-in. Rest. |
| Day 2 | CBCT, intraoral scan, photographs, bloods, anaesthetist consultation |
| Day 3 | Virtual implant plan, surgical guide printed, patient approval |
| Day 4 | Surgery: extractions, ridge modification, four implants, torque verified, PMMA provisional (if ≥35 Ncm) |
| Day 5 | Day 1 post-op: swelling check, hygiene, diet guidance |
| Day 6 | Day 2 post-op: rest |
| Day 7 | Day 3 post-op: bite adjustment, suture review |
| Day 8 | Comprehensive review, photographs, discharge planning |
| Days 9–10 | Final review, fly home |
| Month 4–6 (Visit 2, 5 nights) | Definitive monolithic zirconia prosthesis fitted |
Questions about this procedure?
The 35 Ncm Torque Gate
What is the 35 Ncm torque gate in All-on-4?
> Immediate loading, fitting the same-day provisional, requires a minimum insertion torque of 35 Newton-centimetres at full seating depth on each of the four fixtures. This threshold, established in the original Maló protocol and validated in every subsequent All-on-4 study, ensures sufficient primary stability for the provisional to function without micromotion that would disrupt osseointegration. 5% of cases at Stunning Dentistry, all four fixtures meet the threshold and the provisional is fitted same-day. 5%, one or more fixtures fall short, healing abutments are placed, and the patient returns at month 4 for the fixed provisional. No cost difference.
The 35 Ncm torque gate is the most important single measurement in All-on-4 surgery, and it is the measurement that separates protocol-driven care from outcome-driven shortcuts. Insertion torque reflects the friction between the implant threads and the bone walls at the moment of full seating, it is the closest measurable proxy for primary stability in theatre, and primary stability is the prerequisite for immediate loading.
At Stunning Dentistry, the torque reading is shared with the patient on the day of surgery, not retrospectively in a clinical note. If the reading is 32 Ncm rather than 38, the patient knows, the clinical team knows, and the provisional is not fitted. No same-day provisional is fitted at Stunning Dentistry to meet a patient's schedule expectation rather than to meet the biomechanical threshold.
Ready to discuss your options?

Pain and Sedation
How painful is All-on-4 surgery?
> All-on-4 is performed under local anaesthesia with IV sedation available for all patients, most patients are unaware of the procedure. Post-operative discomfort is mild-to-moderate for 3–5 days, managed with paracetamol plus ibuprofen per the NZ Formulary. Swelling peaks at 48–72 hours. The provisional phase is comfortable. Most patients report the recovery as less difficult than they expected.
All-on-4 surgery is performed under local anaesthesia. IV sedation (Midazolam + Propofol, monitored by an anaesthetist throughout) is available to every patient who requests it and is the standard at Stunning Dentistry for international patients undergoing implant surgery, it eliminates awareness of the procedure without the risks of general anaesthesia. Nitrous oxide inhalation sedation is available as an adjunct for anxious patients who prefer not to be IV-sedated.
At Stunning Dentistry, the pre-surgical protocol includes written sedation consent specifying the anaesthetic agent, monitoring protocol, and discharge criteria. The anxiolysis pathway, Zoom consultation the week before surgery to walk through the day-of-surgery sequence minute-by-minute, is available to any patient who requests it. Surgical anxiety is a clinical reality, not a personal weakness, and the protocol accounts for it explicitly.
Curious about costs and timelines?

Risk Transparency
What are the risks of All-on-4?
> Early implant failure (non-integration within 3 months) occurs in 2–3% of cases, within the published range and replaced at Stunning Dentistry's cost under Category A warranty. Late implant failure (peri-implantitis at 12+ months) occurs in approximately 8% cumulatively at 10 years in published series, with maintenance adherence as the primary modifiable risk factor. PMMA provisional fracture occurs in 4–5% of cases during weeks 1–12 and is replaced within 7 days under warranty. 5% under normal load.
Escalation pathway (New Zealand patients):
Clinical: Ravi Sharma → Clinical Warranty Committee → Australasian prosthodontist consultant (Auckland/Sydney/Melbourne rotating)
| Risk Event | Published Rate | SD Series Rate | Category | Management |
|---|---|---|---|---|
| Early implant failure (non-integration, <3 months) | 2–4% | 2.1% | A, replaced at SD's cost, including re-trip flights | Removal and replacement after 3-month healing |
| Delayed loading (torque <35 Ncm) | 12–14% | 13.5% | Expected, not a failure | Healing abutments; return at month 4 for fixed provisional |
| Provisional (PMMA) fracture (weeks 1–12) | 4–5% | 4–5% | A, replacement within 7 days | In-house replacement |
| Definitive zirconia fracture (normal load) | <0.5% | <0.5% | A | Replacement under documented warranty period |
| Definitive zirconia fracture (bruxism, uncontrolled) | Up to 2% | Variable | B, conditional on documented maintenance | Replacement depends on maintenance record |
| Peri-implantitis (10-year cumulative) | ~8% | Monitored | B, conditional on documented maintenance adherence | Perioperative debridement, antimicrobial protocol |
| Screw loosening | Expected maintenance event | Annual | Not a warranty trigger | Re-torque at annual review |
Want a personalised treatment plan?

Claim Boundaries
What can All-on-4 realistically promise?
6% (Pjetursson, COIR 2012). The Maló Clinic's 18-year longitudinal data (2019) shows 93% cumulative implant survival and 99% prosthetic survival. These are population-level outcomes, individual results are influenced by bone density, occlusal load, smoking status, systemic health, and maintenance compliance. Lifetime implant warranty at Stunning Dentistry covers failure to integrate and premature loss; the prosthetic warranty covers structural defects over the documented warranty period.
All-on-4 outcomes are among the best-documented in implant dentistry. The evidence base spans 25 years and multiple independent institutions. The survival numbers above are from the largest published series. Individual outcomes, however, depend on factors that are measurable before surgery (bone density, HbA1c, smoking status) and on factors that are managed after surgery (maintenance compliance, night-guard use, oral hygiene).
Questions about this procedure?
Clinical Success Determinants
What determines All-on-4 long-term success?
> The five primary determinants: implant primary stability (≥35 Ncm at all four fixtures); surgical guide accuracy (reduces placement error from ±5 mm manual to ±0.3 mm guided); smoking cessation (perioperative and preferably permanent, active smoking doubles late implant failure rate); maintenance compliance (annual reviews, 6-monthly hygiene, nightly night-guard); and systemic health control (HbA1c <8.0% for diabetic patients).
| Determinant | Target | Consequence of Miss |
|---|---|---|
| Primary stability (all 4 fixtures) | ≥35 Ncm | Immediate loading not possible; delayed protocol |
| Surgical guide accuracy | ±0.3 mm (guided) vs ±5 mm (freehand) | Misplaced fixture → compromised A-P spread → cantilever failure |
| Smoking cessation | Complete cessation perioperatively; permanent preferred | Late implant failure rate doubles in active smokers |
| Night-guard use | Every night from provisional delivery | Zirconia fracture risk increases ×3 in unprotected bruxists |
| Maintenance adherence | Annual review, 6-monthly hygiene | Peri-implantitis probability doubles in non-maintained cohorts at 5 years |
| Systemic health (HbA1c) | <8.0% at surgery | Osseointegration failure rate increases above this threshold |
Ready to discuss your options?
Healing Timeline
How long does All-on-4 take to heal?
> Implants osseointegrate over 3–6 months. The PMMA provisional is worn during this period. The definitive monolithic zirconia prosthesis is delivered at month 4–6 on the return trip (5 nights). Post-surgical swelling resolves in 5–7 days. Soft diet applies for weeks 1–12. Full diet resumes after definitive delivery. Marginal bone remodelling continues for 12 months post-placement and is monitored radiographically.
| Timepoint | What Is Happening |
|---|---|
| Day 4 (surgery) | Implants placed; PMMA provisional fitted where ≥35 Ncm |
| Days 5–12 | Swelling resolves; soft diet; initial osseointegration begins |
| Weeks 1–12 | Soft diet (kūmara, eggs, soft fish, yoghurt); bi-weekly Zoom check-ins |
| Month 3 | NZ hygienist visit; Zoom consultation with prosthodontist |
| Month 4–6 | Return to India (5 nights); definitive monolithic zirconia prosthesis delivered |
| Month 12 | Annual review; screw re-torque; radiographic bone-level check |
| Year 5 | Full CBCT bone-level audit; prosthesis renewal review |
| Year 10 | Prosthesis renewal under warranty if warranted |
Curious about costs and timelines?

Retreatment and Alternative Options
What are the alternatives to All-on-4?
> All-on-6: distributes load across six implants, better for bruxism, high bite force, or natural opposing dentition. Zygomatic implants: for severe posterior maxillary atrophy where standard implants cannot be placed. Hybrid FMR: when part of the arch is salvageable and full extraction is unnecessary. Implant-supported overdenture: lower cost, removable, implant-retained, lower function and satisfaction scores than fixed All-on-4 in published QoL comparisons. Complete denture: no implants, lowest cost, lowest function, continued bone loss.
The most common All-on-4 retreatment scenarios are: a failed primary implant replaced after 3-month healing (occurs in 2.1% of the SD series; Category A warranty covers re-trip and replacement); a peri-implantitis case requiring debridement and possibly one implant removal and replacement (occurs in ~8% at 10 years, conditional Category B coverage); and a definitive prosthesis fracture requiring replacement (under 0.5%, Category A).
Want a personalised treatment plan?

Cost Logic, NZD Out-of-Pocket Reality
What is the total NZD cost of All-on-4 at Stunning Dentistry including travel from New Zealand?
> For both arches: NZD 27,500–37,000 clinical fee + NZD 1,300–2,200 return economy flights (from AKL/WLG/CHC) + NZD 700–1,200 hotel (10 nights) + visa (~NZD $40) and travel insurance = approximately NZD 29,500–40,400 total. The equivalent NZ private specialist quote is NZD 68,000–96,000 (clinical fee only). Net saving after all travel costs: NZD 28,000–55,600.
All-on-4 Both Arches, Total NZD Out-of-Pocket
Insurance and funding:
- ACC: not applicable unless dental damage is accident-related. If tooth loss resulted from a covered accident, lodge an ACC45 claim before planning.
- Southern Cross, nib NZ, Accuro, UniMed, Partners Life: Most dental implant procedures are excluded from standard policies. Higher-tier Major Dental benefit caps (NZD 1,000–2,500/year) may partially offset costs. Itemised invoices with NZDA item descriptors issued for all claims.
| Line Item | NZD Range | Notes |
|---|---|---|
| Clinical fee at Stunning Dentistry (both arches) | 27,500–37,000 | All-inclusive: CBCT, guide, surgery, sedation, PMMA provisional, zirconia definitive, post-op, 12-month follow-up |
| Return economy flights (AKL/WLG/CHC ↔ HYD) | 1,300–2,200 | Via Singapore, Kuala Lumpur, Sydney, Dubai, or Doha |
| Hotel (10 nights, 4-star) | 700–1,200 | Partner rate near clinic; airport transfers included |
| India e-Medical Visa | ~40 | Online, 1–3 working days |
| Travel insurance | 200–450 | NZ-based provider; confirm international medical coverage |
| **Total NZ out-of-pocket (both arches)** | **~NZD 29,740–40,890** | All-inclusive |
| NZ private specialist quote (both arches) | 68,000–96,000 | Clinical fee only, no travel |
| **Net saving** | **~NZD 28,000–55,000** | After all travel costs |
Questions about this procedure?
Comparison Matrix
How does All-on-4 compare to All-on-6, zygomatic implants, and dentures?
6% 10-year implant survival in most full-arch patients. All-on-6 adds two implants for better load distribution, preferred for bruxism and high bite force. Zygomatic implants are for severe maxillary bone loss where no standard protocol applies. Complete dentures carry the lowest function, lowest satisfaction, and accelerate ongoing bone loss. The right choice is driven by bone volume, bite force, and the proportion of viable natural teeth.
| Option | Fixed/Removable | Implants | 10-Year Survival | SD Cost (NZD, both arches) | Best For |
|---|---|---|---|---|---|
| All-on-4 | Fixed | 4 per arch | 94.6% implant survival | 27,500–37,000 (total w. travel: ~30,000–40,000) | Most full-arch patients; moderate posterior atrophy |
| All-on-6 | Fixed | 6 per arch | 95–97% implant survival | 32,000–44,000 (total w. travel: ~35,000–47,000) | Bruxism; high bite force; natural opposing dentition |
| Zygomatic | Fixed | 2–4 zygomatic + 2 anterior | 90–95% at 10 years | 32,000–44,000 (total w. travel: ~35,000–47,000) | Severe posterior maxillary atrophy; failed grafts |
| Implant overdenture | Removable/retained | 2–4 per arch | 95% implant survival | 16,000–24,000 | Budget-constrained; removable acceptable |
| Complete denture | Removable | 0 | N/A | 2,000–5,000 | Medical contraindication to surgery |
Ready to discuss your options?
Post-Treatment Biological Reality
What happens biologically after All-on-4 is complete?
> Osseointegration completes over 3–6 months. Marginal bone remodelling around the four fixtures continues for 12 months post-placement. 2 mm per year thereafter in maintained cases. 3 mm, within biological function thresholds. Night-guard use prevents zirconia fracture and reduces cantilever stress. Annual radiographic monitoring confirms bone-level stability.
The All-on-4 prosthesis functions as a biological prosthesis after delivery, it loads the bone through the four fixtures, it is cleaned around the gingival margins daily, and it is monitored annually for bone-level stability. Three things keep it working for 15+ years: night-guard use every night, professional hygiene every 6 months, and annual radiographic bone-level review.
At Stunning Dentistry, the biological reality of year 8 is as well-documented in the patient file as the reality of day 4. The 924-case cohort includes patients at year 12 and year 15 of follow-up. What is observed at those timepoints is what the post-treatment protocol is designed to produce: bone levels within the Albrektsson threshold, screw integrity maintained by annual re-torque, and prosthetic surfaces showing measurable but clinically insignificant wear. The protocol produces the outcome. The outcome requires the protocol.
Curious about costs and timelines?
Common Mistakes
What are the most common mistakes with All-on-4?
> The three most common: choosing a clinic based on price without verifying the implant brand and surgical guide protocol; not respecting the soft-diet calendar during the provisional phase (risks micromotion at the implant-bone interface); and failing to build a NZ hygienist relationship for the maintenance phase. A fourth, specific to clinics, not patients, is fitting the provisional below the 35 Ncm threshold to meet the patient's same-day expectation.
The most consequential mistake in the All-on-4 market is choosing a clinic based on price without verifying the implant brand, the surgical guide protocol, and the written warranty. An All-on-4 at 50% of the standard cost typically means unlisted implants (no 10-year published data), freehand surgery (±5 mm placement error vs ±0.3 mm guided), and a verbal warranty. The patient will not know the difference on day 4 in India. They will know the difference at month 24 in Auckland.
At Stunning Dentistry, every NZ patient leaves with a written 10-year maintenance calendar, annual review dates, hygienist visit schedule, night-guard replacement milestone, screw re-torque protocol, and the radiographic upload instructions for the annual Zoom review. The calendar is not aspirational; it is part of the clinical record.
Want a personalised treatment plan?
Myth Deconstruction
What are the most common All-on-4 myths?
> Myth 1: The day-1 bridge is your final teeth. False, the PMMA provisional is a 4-6-month temporary; the definitive monolithic zirconia is fitted on the return trip. Myth 2: You can fly home the next day. False, a minimum 4–5 days in Hyderabad post-surgery is the clinical protocol; 72-hour no-fly minimum for sinus-adjacent placements. Myth 3: All implant clinics use the same implants. False, Straumann and Nobel Biocare have 25+ years of published data; unknown-brand implants do not. Myth 4: All-on-4 is always better than All-on-6. False, for bruxism and high bite force, All-on-6 reduces cantilever stress and fracture risk.
The PMMA provisional bridge fitted on Day 4 is my final teeth.**
No. The PMMA provisional is a diagnostic and functional temporary worn during the 4–6-month osseointegration period. It is metal-reinforced, milled, and warrantied for 1 year, it is a high-quality temporary, not a cheap placeholder. The definitive monolithic zirconia prosthesis, warranted for 10 years against fracture under normal load, is fitted on the return trip at month 4–6.
I can fly home the next day after All-on-4 surgery.**
The clinical protocol at Stunning Dentistry requires a minimum 4–5 days in Hyderabad post-surgery. For implants placed adjacent to the sinus floor, a 72-hour no-fly minimum applies. The reason is not administrative, it is clinical. Post-surgical swelling, bite adjustment, and the first 48-hour healing window need in-person review. Flying with active post-surgical swelling in a pressurised cabin at 38,000 feet is a comfort and complication risk.
All implant clinics offering All-on-4 use equivalent implants.**
Straumann SLActive and Nobel Biocare NobelActive have published 25-year survival data and independent third-party validation. Unknown-brand implants may have acceptable short-term results; they have no independent 10-year data, no international distribution network, and no Australasian support infrastructure. The difference matters at year 8 when a New Zealand implantologist needs to service the components.
All-on-4 is always superior to All-on-6.**
All-on-4 is the appropriate choice for most full-arch patients, it avoids sinus grafts, reduces surgical complexity, and has the best published evidence base. For documented bruxism, natural opposing dentition generating high occlusal forces, or a patient with a history of prosthetic fracture, All-on-6 distributes load across a wider platform, reduces the cantilever moment on the distal fixtures, and produces lower zirconia fracture rates. The choice is biomechanical, not promotional.
Questions about this procedure?
People Also Ask
Will I leave India with fixed teeth?
The Maló Clinic's 18-year data shows 93% cumulative implant survival and 99% prosthetic survival. Individual outcomes depend on bone quality, maintenance adherence, smoking status, and systemic health. With nightly night-guard use, 6-monthly hygiene, and annual review, most All-on-4 restorations function well beyond 15 years.
Ready to discuss your options?

Ask Your Doctor
Bring these questions to any All-on-4 consultation, at Stunning Dentistry or anywhere else.
1. What implant brand and specific system will you use, Straumann SLActive, Nobel Biocare NobelActive, Osstem? Can I see the manufacturer data?
2. Will surgery be guided (printed surgical guide from CBCT plan) or freehand?
3. What is the 35 Ncm threshold policy, will you fit the provisional if any fixture falls below threshold?
4. What happens if I leave with healing abutments rather than a provisional, what are the cost and trip implications?
5. What is the written warranty, on the implants, the PMMA provisional, and the zirconia definitive?
6. Who is the lead implantologist, and how many All-on-4 cases do they perform annually?
7. What is the post-operative protocol for the return flight home, minimum days in India post-surgery?
8. How will I be followed up in New Zealand, who contacts who, at what intervals, and what is the escalation path if I have a prosthetic concern?
9. What is the soft-diet protocol, and for how long?
10. What happens if an implant fails to integrate, re-trip, cost, timeline?
Curious about costs and timelines?
Want a personalised treatment plan?
Book a Consultation
If you are unsure whether All-on-4 is the right treatment, or whether the India pathway makes sense for your case, request a remote CBCT review.
Diagnosis precedes decision.
Questions about this procedure?

Ready to discuss your options?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Can my NZ dentist refer me for an All-on-4 review before I commit?
Yes. We accept CBCT in DICOM format (taken by your NZ dentist, dental radiologist, or hospital radiology department) for remote review. If no CBCT exists, a panoramic (OPG) is sufficient for a preliminary assessment, the full plan requires CBCT. DICOM files can be sent through our clinical portal; we provide a written review within 5 business days.
What if my NZ dentist quoted me for All-on-6 or zygomatic?
Send us the CBCT and the NZ quote. We re-plan honestly. In 9% of quoted All-on-6 cases, All-on-4 is adequate for the bone and bite-force profile. In 6% of quoted zygomatic cases, All-on-4 is adequate. The inverse, NZ-quoted All-on-4 that requires zygomatic, occurs in 6% of our remote review cases. Plan follows diagnosis.
What if I have a problem in New Zealand 2 years after treatment?
Contact Ella Watson (CRM manager, 24/7) immediately. Average initial response time: under 30 minutes during business hours. Same-day Zoom triage with the assigned clinician. Escalation to a New Zealand specialist partner for in-person assessment where needed, with all clinical records shared and the visit covered under warranty terms.
Can I eat normally after the definitive zirconia is fitted?
Yes, with the standard long-term precautions for any fixed prosthesis: no ice-chewing, no biting hard objects with the anterior teeth, no bones, and nightly night-guard use. These precautions apply for the life of the prosthesis.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.