Full Mouth Rehabilitation for New Zealand Patients, The Complete Clinical Guide
- What Full Mouth Rehabilitation Actually Is

Full-Arch Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Immediate Load
Full-arch or multiple implant cases where provisional teeth are placed shortly after surgery in suitable clinical conditions.

Multiple Implant Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.

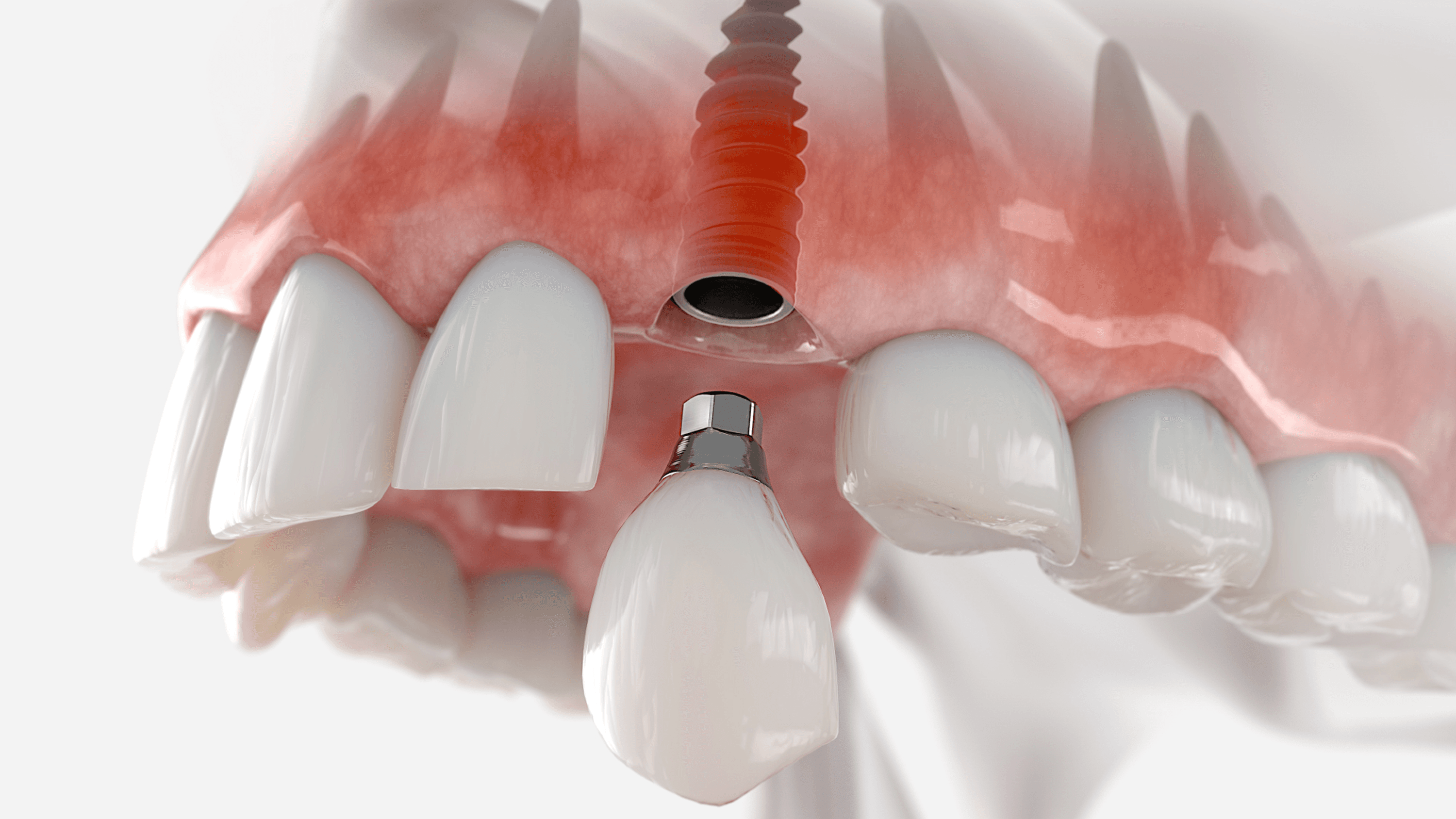
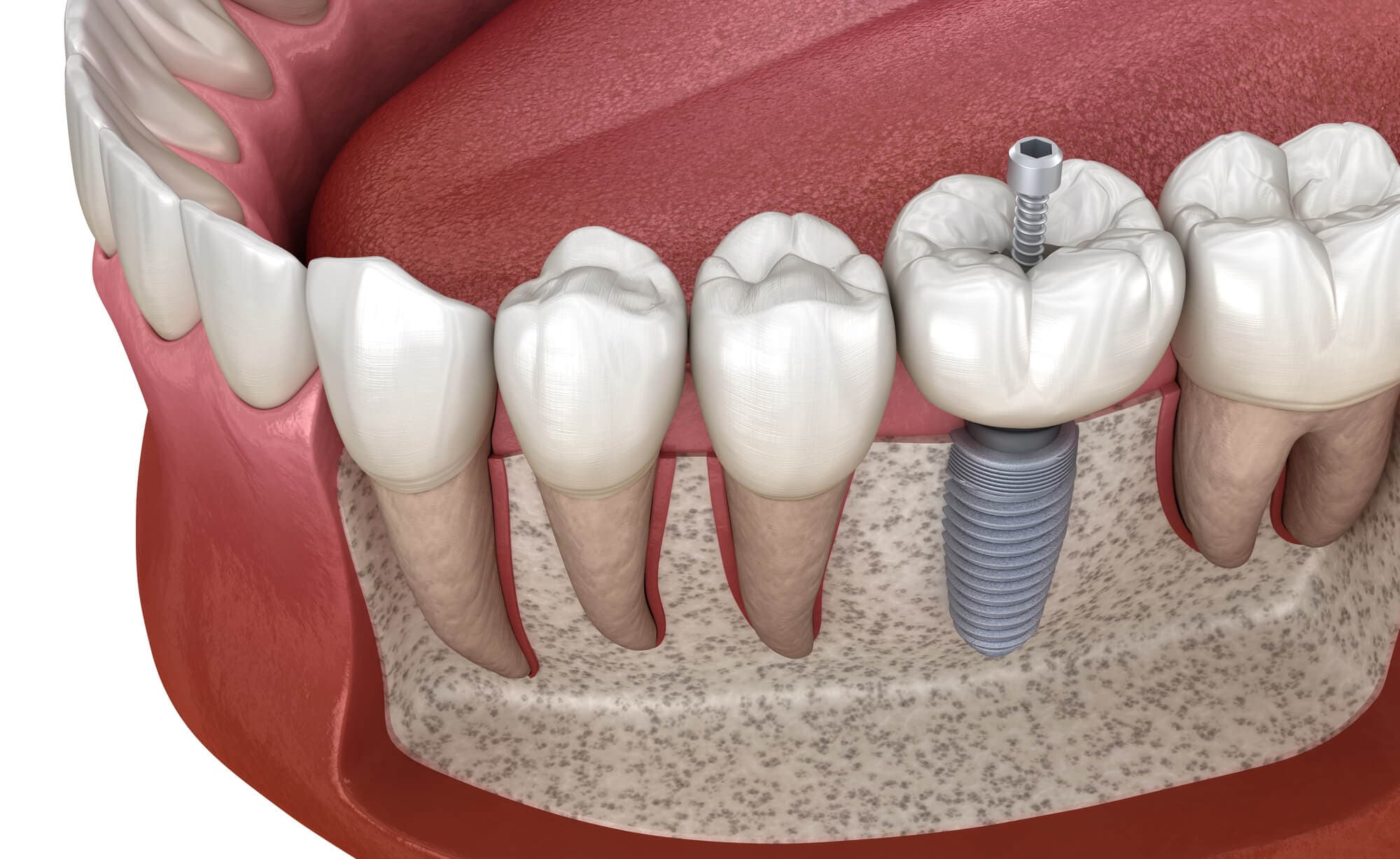
Single Tooth Implant
Single-tooth replacement with an implant and crown for a natural-looking, long-lasting result.

Bone Grafting & Advanced Surgical Support
Regenerative procedures performed to establish adequate bone volume for stable implant placement.
Revision & Complex Implant Cases
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Is Full Mouth Rehabilitation What You Actually Need?
Is full mouth rehabilitation what you actually need?
> Full mouth rehabilitation is the coordinated, sequenced rebuilding of every occlusal surface, every missing tooth site, and the underlying vertical dimension across one or both arches. It is indicated when individual-tooth dentistry can no longer restore function. Most cases in New Zealand take 9–18 months and cost NZD 92,000–150,000 privately. The same treatment at Stunning Dentistry in India costs NZD 37,000–68,000 total including return flights from Auckland, Wellington, or Christchurch.
Full mouth rehabilitation is the category of dentistry that begins where individual-tooth treatment ends. When a New Zealand prosthodontist traces a pattern of systemic wear on a CBCT, when a periodontist explains that no single tooth is the structural problem, when a Wellington or Auckland GDP says "you've outgrown what I can offer", that is the moment FMR becomes the conversation.
For patients reading from Aotearoa New Zealand: the FMR available here operates under the same internationally recognised frameworks, Dawson, Kois, Pankey, Spear, Hobo-Takayama, taught to prosthodontists on the Dental Council of New Zealand (DCNZ) Specialist List. The diagnostic protocols, material standards, and implant systems are internationally consistent. What changes when you travel to Stunning Dentistry is not the clinical protocol, it is the depth of the specialist bench on every case, the in-house digital infrastructure, and the total cost against NZD private-practice quotations.
The saving after full travel costs is NZD 50,000–85,000 depending on scope and case complexity.
| FMR Pathway | Duration | NZD Cost Range | Notes |
|---|---|---|---|
| Tooth-supported (NZ private specialist) | 9–12 months | 50,000–130,000 | Clinical fee only |
| Implant-supported / hybrid (NZ private specialist) | 12–18 months | 65,000–150,000 | Clinical fee only |
| Tooth-supported FMR at Stunning Dentistry | 9–12 months | 37,300–56,650 | Total incl. 2 return trips, hotel, visa |
| Implant-supported (All-on-4 dual arch) at SD | 4–6 months | 25,400–37,000 | Total incl. travel |
| Complex multi-phase (implants + ortho + perio) | 14–18 months | 42,200–67,600 | Total incl. 3 return trips |
Questions about this procedure?
What Full Mouth Rehabilitation Actually Is
What is full mouth rehabilitation?
> Full mouth rehabilitation is the simultaneous or staged restoration of every occlusal surface, every missing tooth site, and the underlying vertical dimension and periodontal foundation across one or both arches in a single coordinated treatment plan. The operative word is coordinated, twelve crowns placed across twelve individual appointments is not FMR. One integrated plan, one articulator mounting, one named clinical team, is.
Full mouth rehabilitation is the simultaneous or staged restoration of every occlusal surface, every missing tooth site, and the underlying vertical dimension and periodontal foundation across one or both arches, in a single, coordinated treatment plan. The operative word is coordinated. A patient who receives twelve individual crowns from twelve individual planning sessions has not had an FMR. A patient whose crowns, implants, orthodontics, and occlusal design were planned on a single articulator mounting, executed in a single sequenced protocol, and verified through a common provisional phase has had an FMR.
Three Structural Modalities of FMR
| Modality | Used When | Key Feature |
|---|---|---|
| Tooth-supported | Dentition preserved but worn or restoratively compromised | Crowns, onlays, veneers, bridges on natural teeth |
| Implant-supported | Dentition is terminal (All-on-4, All-on-6, zygomatic, full-arch fixed) | Strategic clearance, implant-borne prostheses |
| Hybrid | Parts of the arch can be saved, parts cannot | Tooth and implant coexist in the same arch |
Ready to discuss your options?

The Diagnostic Frameworks That Govern the Rebuild
What diagnostic frameworks govern full mouth rehabilitation?
> Four internationally recognised frameworks, Dawson, Kois, Pankey, and Hobo-Takayama, are used to plan FMR. Each solves a different clinical problem: Dawson addresses CR-MIP discrepancy; Kois structures risk stratification; Pankey emphasises the diagnostic provisional; Hobo-Takayama builds the occlusion against actual condylar guidance. The framework is assigned at the first consultation, not chosen mid-treatment.
Every full mouth rehabilitation runs on a named diagnostic framework. The framework is chosen on case presentation, not clinic preference. The four frameworks used at Stunning Dentistry, and what each is designed to solve, are described below.
At Stunning Dentistry, the Spear Education protocols, which sit alongside the four classical frameworks as a modern integration model, are cross-referenced against the primary framework on every multi-discipline case. Spear's Facially Generated Treatment Planning integrates orthodontic, periodontal, and restorative decisions against a single facial reference, compressing the design iteration that used to take weeks into a single digital planning session.
| Framework | Best Used For | Defining Feature |
|---|---|---|
| Dawson | Collapsed bite, CR-MIP slide >2 mm | Bimanual CR verification, articulator-based bite recording |
| Kois | Aesthetic-led cases, complex risk profiles | Six-domain risk stratification before restorative work begins |
| Pankey | Bruxism, behavioural complexity, long provisional need | Long provisional phase as primary diagnostic instrument |
| Hobo-Takayama | Steep condylar guidance, bruxism, post-orthodontic | Twin-stage construction, posterior cusp height first, anterior guidance second |
| Spear | Multi-discipline integration, facially driven design | Facially Generated Treatment Planning, digital iteration |
Curious about costs and timelines?

Who Is a Candidate, And Who Isn't
Who is a candidate for full mouth rehabilitation?
> Strong candidates have failing full arches or systemic dentition collapse where individual-tooth work can no longer restore function. Minimum requirements: adequate bone foundation (or implantable bone), medically fit for the chosen procedure, and realistic about the 9–18 month treatment arc. Patients with active uncontrolled systemic disease, heavy unaddressed bruxism, or insufficient travel availability for a multi-visit India pathway should be assessed individually before committing.
Full mouth rehabilitation is indicated when the dentition has reached the threshold where individual-tooth work can no longer restore function. The realistic alternative choices are: continued patchwork repair (which typically ends in emergency extractions over 5–10 years), acceptance of removable dentures, or a planned rehabilitation. The clinical decision is made on the pattern of failure, not on the number of teeth involved.
Candidacy Assessment Summary
| Profile | Candidacy | Next Step |
|---|---|---|
| Failing full arch, adequate anterior bone, non-smoker, fit for sedation | Strong candidate | Book diagnostic CBCT review |
| Documented bruxism, natural opposing dentition, high occlusal forces | Consider All-on-6 or Hobo-framework approach | Discuss load distribution at consultation |
| Severe posterior maxillary atrophy (ZAGA III–IV, <4 mm posterior bone) | Consider zygomatic implants | Zygomatic protocol assessment |
| Active uncontrolled diabetes (HbA1c >8.5%) | Not recommended until systemic control | Medical management first |
| Recent (<2 years) head/neck radiotherapy | Contraindicated for implant-supported FMR | Tooth-supported evaluation only |
| Active heavy smoking, unwilling to abstain | High-risk, implant component only | Informed decision with documented risk |
| Cannot commit to 3–5 weeks across 2–3 India visits | India pathway not suitable | NZ specialist pathway recommended |
Want a personalised treatment plan?
When NOT to Choose Full Mouth Rehabilitation
When is full mouth rehabilitation not the right choice?
> FMR is not indicated for localised or single-quadrant problems, for active systemic disease that precludes surgery, or for patients unable to commit to the multi-visit timeline. The threshold to declare an FMR case is deliberately high, a patient with severe wear on the anterior sextant may be better served by composite build-ups, a Michigan splint, and a 6-month review. The distinction matters because FMR is a 9–18-month commitment.
Full mouth rehabilitation is not the correct treatment for every failing dentition. The most common overdiagnosis in comprehensive dentistry is an FMR being declared for a case that could be managed with a conservative, localised approach, and the harm is significant: unnecessary expense, unnecessary tooth reduction, unnecessary commitment to a decades-long maintenance relationship.
- Systemic dentition collapse, multiple arches, multiple modalities required
- VDO loss >2 mm, CR-MIP discrepancy requiring full-arch provisional testing
- Terminal dentition with implant rehabilitation as the primary modality
- Congenital enamel disorders (amelogenesis imperfecta, dentinogenesis imperfecta)
- Post-oncology or post-trauma full-arch reconstruction
Do NOT Choose FMR When:
- Localised anterior wear manageable with composites and a splint
- Isolated quadrant failure where segmental crown-and-bridge is appropriate
- Active systemic disease contraindicating surgery (uncontrolled diabetes, recent radiotherapy)
- Patient cannot commit to 2–3 India visits across 9–18 months
- Savings after honest travel-cost accounting are under NZD 12,000
Questions about this procedure?

Step-by-Step: How Full Mouth Rehabilitation Is Performed
How is full mouth rehabilitation performed step by step?
> FMR is delivered in four main phases: diagnostic (CBCT, articulator mounting, digital wax-up, mock-up preview); preparatory (periodontal therapy, extractions, implant surgery where indicated, provisional restorations placed); definitive fabrication (impressions or scans, in-house milling, try-in, cementation or screw retention); and long-term maintenance (annual reviews, Zoom follow-up, NZ hygienist network). Total treatment time: 9–18 months. India visits: 2–3 trips.
The FMR pathway begins with the diagnostic phase and ends only at the long-term maintenance review, not at the delivery of the definitive restorations. Every step between those two endpoints is governed by the assigned framework and the SD-FMR-05 protocol.
Phase 1, Diagnostic (Days 1–3 of Visit 1, India): Full CBCT, intraoral scanning (iTero or Medit i700), periodontal charting, facebow-assisted bite registration in centric relation. Articulator mounting, Panadent PCH, Whip Mix 8500, or Artex CR depending on case. Digital wax-up in exocad DentalCAD. Mock-up preview (Trial Smile), the patient sees the planned outcome before committing. Multi-specialist case review with lead prosthodontist, implantologist, and periodontist. Treatment plan signed after patient approval.
Phase 2, Preparatory and Surgical (Days 4–5 of Visit 1): Periodontal therapy for any active disease. Endodontic treatment on foundational teeth. Strategic extractions where indicated. Implant placement under local anaesthesia with IV sedation or nitrous oxide, fixtures placed through printed surgical guide, torque verified per-fixture. Provisional restorations placed at the same session. Patient discharged home with written aftercare protocol and named CRM manager contact.
Phase 3, Provisional (3–6 months, remote from New Zealand): The provisional phase is not a waiting period, it is a diagnostic phase. The patient tests the new VDO, the new CR, the new anterior guidance, and the new aesthetic outcome in their real daily environment. Weekly hygiene photo uploads during month 1, bi-weekly Zoom check-ins with the assigned prosthodontist for the first 8 weeks, monthly thereafter.
Phase 4, Definitive Fabrication and Delivery (Visit 2, India, 10 days): Provisional phase reviewed, VDO and occlusion verified. Final digital impressions. In-house CAD/CAM milling and sintering during the visit, no external lab dependency, no additional wait. Try-in for aesthetics, phonetics, and bite. Definitive delivery: cementation or screw retention. Occlusal equilibration. Night-guard fitting. Warranty documentation issued.
At Stunning Dentistry, the in-house infrastructure that makes the definitive fabrication happen within Visit 2, the milling unit, the sintering oven, the characterisation bench, sits in the same building as the operatories. That physical co-location is not a luxury; it is the structural reason a 10-day visit can accomplish what an externally-labed pathway cannot.
Visit Schedule for NZ Patients
| Visit | Duration | What Happens | When |
|---|---|---|---|
| Visit 1 | 10 days | Diagnostic, preparatory, surgical, provisional | Week 1 of treatment |
| Between visits | 3–6 months | Provisional phase, Zoom follow-up, NZ hygienist | At home in New Zealand |
| Visit 2 | 10 days | Provisional review, definitive fabrication, delivery | 3–6 months after Visit 1 |
| Visit 3 (complex cases) | 5 days | 12-month audit, component refinement, clinical sign-off | 12 months after Visit 2 |
Ready to discuss your options?
Pain and Sedation
How painful is full mouth rehabilitation?
> Individual phases are managed under local anaesthesia. IV sedation and inhalation sedation (nitrous oxide) are available for surgical phases. Most patients report mild soreness for 2–3 days after each preparation or surgical phase, managed with paracetamol plus ibuprofen per the NZ Formulary. The provisional phase is comfortable. Speech adaptation to new anterior positions takes 2–4 weeks and resolves before the definitive is seated.
Pain management in FMR is staged to the procedure. The preparatory phase, extractions, ridge modification, implant surgery, uses local anaesthesia as the primary modality with IV sedation or nitrous oxide inhalation sedation available for any patient who requests it or for whom the surgical complexity justifies it. No phase of FMR at Stunning Dentistry requires general anaesthesia.
At Stunning Dentistry, our pre-surgical protocol includes anxiolysis guidance for patients with dental anxiety, pre-operative Zoom consultation to walk through the day-of-surgery sequence, and a written sedation consent form that specifies the anaesthetic agent, the monitoring protocol, and the discharge criteria. No surgical phase proceeds without the patient understanding each step in advance.
| Phase | Pain Level | Management | Duration |
|---|---|---|---|
| Diagnostic (CBCT, scans, impression) | None | None required | Days 1–3 |
| Preparatory (extractions, ridge work) | Mild post-op | Paracetamol + ibuprofen, per NZ Formulary | 2–3 days |
| Implant surgery | Mild-to-moderate post-op | LA + IV sedation or nitrous; oral analgesics post-op | 3–5 days |
| Provisional restorations | None to mild | Occlusal adjustment if needed | Immediate |
| Definitive delivery | None | None required | , |
| Adaptation (speech, bite) | Nil pain, cognitive | Normal adaptation; resolves in 2–4 weeks | 2–4 weeks |
Curious about costs and timelines?

Risk Transparency
What are the risks of full mouth rehabilitation?
> Published 10-year mechanical complication rates for FMR range from 20–35%. The most common events are screw loosening (manageable remotely), provisional fracture (replaced without structural impact), crown chipping on a definitive (repaired or replaced under warranty), and peri-implantitis in implant-supported components (~5% at 10 years in compliant patients). Severe biological complications, implant failure, prosthetic structural failure, occur in under 5% of well-planned, well-maintained cases.
Full mouth rehabilitation carries documented complication rates over a 10-year horizon that every patient should understand before committing. The complication rate should not be treated as a reason to avoid FMR, the alternative of untreated systemic dentition collapse carries a higher long-term burden, but it should be treated as a reason to choose the right clinical framework, the right implant system, and the right follow-up protocol.
At Stunning Dentistry, every FMR patient receives a written complication protocol at consent, specifying the most common events by frequency, the response pathway for each (remote management, referral to a New Zealand provider, return visit to India), and the warranty coverage that applies. A clinician who claims a zero-complication rate for FMR is not being honest. Published rates are 20–35% mechanical over 10 years. Knowing what to expect and how it will be handled is more protective than being told everything will be fine.
| Complication | Frequency | Management | Covered by Warranty |
|---|---|---|---|
| Screw loosening | Most common mechanical event | Remote tightening at review visit | Yes |
| Provisional fracture | Common during provisional phase | Replacement, no structural impact | Yes |
| Crown chip / minor fracture | Occasional | Repair or replacement | Yes |
| Peri-implantitis | ~5% at 10 years (compliant patients) | Perioperative debridement, antimicrobial protocol | Covered for treatment-related cases |
| Implant non-integration | 2–4% primary failure rate | Removal and replacement after healing | Yes (lifetime warranty) |
| Prosthetic structural failure | <2% at 10 years | Replacement under documented warranty period | Yes |
| VDO or CR instability (ill-designed provisional) | Preventable by correct provisional protocol | Provisional adjustment; no impact on definitive | Included in provisional phase |
Want a personalised treatment plan?

Claim Boundaries
What can full mouth rehabilitation realistically promise?
6% (Pjetursson, 2012). 18-year prosthetic survival for All-on-4 is 99% (Maló, 2019). Tooth-supported crowns in rehabilitation contexts survive 85–92% at 10 years. These are population-level outcomes, not individual guarantees. Individual outcomes are influenced by bone quality, occlusal load, systemic health, and maintenance compliance. No reputable clinician promises 100% success.
Full mouth rehabilitation outcomes are reported in two separate layers: the implant layer and the prosthetic-unit layer. Both have strong long-term published data. Neither carries a 100% guarantee, and any clinic that offers one should be treated with scepticism.
At Stunning Dentistry, the warranty structure reflects these published numbers. Lifetime warranty on implants covers failure to integrate and premature loss. The prosthetic warranty covers documented material defects and structural failure across the warranty period. What is not covered: damage from wilful neglect, failure to attend maintenance reviews, or the natural wear expected in any restoration under years of occlusal loading. The warranty document is issued in writing at definitive delivery. The fine print is readable.
Questions about this procedure?

Clinical Success Determinants
What determines whether full mouth rehabilitation succeeds long-term?
> The five primary success determinants are: bone quality and implant primary stability (>35 Ncm torque at placement); framework selection matched to the clinical presentation; provisional phase compliance (minimum 6 weeks); maintenance adherence (annual reviews, nightly night-guard use, professional hygiene every 6 months); and systemic health control (HbA1c <8.0% for diabetic patients, complete smoking cessation for implant-supported cases).
Primary Success Determinants
| Determinant | Target | Why It Matters |
|---|---|---|
| Bone quality / implant primary stability | >35 Ncm torque at placement | Threshold for immediate-loading provisional; below this, delayed loading required |
| Framework selection | Matched to CR-MIP discrepancy, bruxism status, and aesthetic complexity | Wrong framework = unsalvageable bite issues post-definitive |
| Provisional phase duration | Minimum 6 weeks; 12 weeks for bruxism cases | VDO and CR must be biologically and neurologically verified before committing in zirconia |
| Maintenance adherence | Annual review, 6-monthly hygiene, nightly night-guard | Mechanical complication rate doubles in non-maintained cohorts at 5-year follow-up |
| Systemic health | HbA1c <8.0%, smoking cessation for implant components | Peri-implantitis risk increases 2–3× in uncontrolled diabetics and active smokers |
| Operator experience | Named specialist team, 100+ FMR cases per year | Complication management and framework precision are experiential, not just academic |
Ready to discuss your options?

Healing and Phasing Timeline
How long does full mouth rehabilitation take to heal?
> Implants osseointegrate over 3–6 months. The provisional phase runs concurrent with this healing and lasts 6–12 weeks minimum. Definitive restorations are delivered after osseointegration is confirmed and the provisional bite approved. Total arc from first surgery to definitive delivery: 4–6 months for implant-supported FMR; 9–12 months for tooth-supported FMR; 14–18 months for complex multi-phase cases. Post-definitive soft-diet precautions last 48 hours.
Recovery at home (post-surgery, provisional phase): Soft diet for 12 weeks. Avoid ice, bones, hard candy, and biting on anything structurally harder than cooked food. Night-guard use nightly from day of provisional delivery. Weekly hygiene photo uploads. Bi-weekly Zoom check-ins with your prosthodontist for the first 8 weeks.
| Phase | Timeline | What Is Happening Biologically |
|---|---|---|
| Post-extraction healing | 0–3 months (if required) | Socket remodelling; bone fill begins at 3–4 weeks, mature at 3 months |
| Implant osseointegration | 3–6 months | BIC (bone-implant contact) accrues from ~25% at placement to >70% at 3 months |
| Provisional phase | 6–12 weeks minimum | Occlusal adaptation, VDO tolerance testing, soft tissue maturation around gingival margins |
| Definitive fabrication | 4 days (in-house milling during Visit 2) | CAD/CAM milling, sintering, characterisation, staining |
| Post-definitive adaptation | 2–4 weeks | Neuromuscular habituation to new occlusal contacts and anterior guidance |
| Year 1 healing | Ongoing | Continued marginal bone remodelling around implants; radiographic stability typically by month 12 |
| Long-term (Year 1–10) | Annual monitoring | Wear assessment, screw retightening, hygiene maintenance |
Curious about costs and timelines?

Retreatment and Alternative Options
What are the alternatives to full mouth rehabilitation?
> The three realistic alternatives to FMR are: continued patchwork repair (replacing individual failing components as they fail, extends function 5–10 years but typically ends in emergency extractions); complete removable dentures (immediate, lower cost, but significantly lower function and patient-reported quality of life); and full-arch implant rehabilitation as a stand-alone (All-on-4, All-on-6, appropriate when the dentition is fully terminal rather than partially salvageable). The choice depends on the proportion of salvageable teeth and the patient's timeline.
Not every patient arriving at an FMR consultation should leave with an FMR treatment plan. The alternatives are legitimate, the choice is clinical, and the honest version of each option is worth understanding before committing to the 9–18 month arc.
At Stunning Dentistry, we recommend FMR only when the case genuinely requires it. Patients arriving with an FMR quote from a New Zealand specialist are screened against this framework at the remote CBCT review, and approximately 12% are redirected to a simpler or more appropriate pathway before their first India visit.
Want a personalised treatment plan?

Cost Logic, NZD Out-of-Pocket Reality
What does full mouth rehabilitation cost in NZD, including all travel?
> Total NZD out-of-pocket for dual-arch tooth-supported FMR at Stunning Dentistry: NZD 37,300–56,650 (including two return trips from Auckland/Wellington/Christchurch, hotel, visa, and companion travel). The equivalent private specialist quote in New Zealand is NZD 92,000–130,000 (clinical fee only). Net saving: NZD 50,000–80,000 after all travel costs. For dual-arch All-on-4 the total including travel is NZD 25,400–37,000 against NZD 60,000–80,000 in New Zealand.
The only number that matters for a New Zealand patient is the total out-of-pocket figure, not the clinical fee alone. Dental-tourism comparisons that quote only clinical fees produce misleading conclusions. The honest comparison is total cost (India: clinical fee + flights + hotel + visa + insurance + companion) versus total cost (New Zealand: clinical fee, no travel overhead).
- Te Whatu Ora / Health New Zealand: Does not fund adult full mouth rehabilitation. Emergency pain-relief only.
- ACC: Accident-related dental only. Wear, erosion, periodontal loss, not covered. If you have a documented accident component, lodge an ACC45 claim before planning.
- Private health insurance (Southern Cross, nib NZ, Accuro, UniMed, Partners Life): Annual caps of NZD 1,000–2,500 on Major Dental cover. Expect to recover 3–10% of the total FMR cost. Itemised invoices with NZDA item descriptors are issued for all claim submissions.
*Cost figures current as of May 2026. Confirmed at consultation.*
| Line Item | NZD Range |
|---|---|
| Clinical fee at Stunning Dentistry | 35,000–55,000 |
| Flights, hotel, visa, transport (three visits) | 5,500–9,800 |
| Companion travel (optional) | 1,700–2,800 |
| **Total NZ out-of-pocket** | **NZD 42,200–67,600** |
| Equivalent NZ quote | **NZD 98,000–150,000** |
| **Net saving** | **NZD 50,000–85,000** |
Questions about this procedure?
Comparison Matrix: FMR vs Alternatives
How does full mouth rehabilitation compare to alternatives?
> FMR delivers fixed, natural-feeling teeth with the highest long-term function score of any reconstruction modality. All-on-4 per arch is the most appropriate simplification for fully terminal dentitions. Patchwork repair is appropriate for stable arches with isolated failures. Complete dentures carry the lowest patient-reported quality of life and accelerate bone loss. The right choice is driven by the proportion of viable teeth, bone volume, and the patient's timeline.
The comparison above uses clinical fee totals at Stunning Dentistry including travel. New Zealand private-practice equivalents are 2.5–4× higher across all modalities except complete dentures.
| Option | Fixed/Removable | 10-Year Survival | NZD Cost (SD, total incl. travel) | Best For |
|---|---|---|---|---|
| Full mouth rehabilitation (tooth-supported) | Fixed | 85–92% as system | 37,300–56,650 | Partially salvageable dentition, VDO collapse, systemic wear |
| All-on-4 per arch | Fixed | 94.6% implant survival | 25,400–37,000 (dual arch) | Terminal dentition, fastest to fixed result |
| All-on-6 per arch | Fixed | 95–97% implant survival | 28,000–40,000 (dual arch) | High bite force, bruxism, natural opposing dentition |
| Zygomatic implants | Fixed | 90–95% at 10 years | 28,000–42,000 (dual arch) | Severe posterior maxillary atrophy, failed grafts |
| Implant-supported denture | Removable/Implant-retained | 95% implant survival; denture replaced every 5–7 years | 14,000–20,000 (dual arch) | Budget-constrained; some stability over full denture |
| Complete removable dentures | Removable | N/A (no implants) | 2,000–5,000 | Medical contraindication to surgery; temporary solution |
| Patchwork repair | Fixed (ad hoc) | Dependent on remaining teeth | Variable, NZ ongoing cost | Stable arch with isolated failing components |
Ready to discuss your options?
Post-Treatment Biological Reality
What happens biologically after full mouth rehabilitation is complete?
> Marginal bone remodelling around implants continues for 12 months post-placement, with radiographic stability typically confirmed by the 12-month review. Soft tissue maturation around crown margins completes at 3–6 months post-definitive. Occlusal wear on prosthetic materials is measurable but clinically insignificant at 10 years in maintained cases. The restoration functions as a biological prosthesis, it requires nightly protection (night-guard), professional maintenance every 6 months, and annual clinical monitoring.
Post-FMR biology is not static. The prosthesis and the tissues around it continue to remodel, adapt, and, without maintenance, deteriorate. Understanding what happens after the definitive is seated is as important as understanding what happens before it.
At Stunning Dentistry, every FMR patient receives a structured maintenance contract: annual Zoom reviews with the assigned prosthodontist, 6-monthly professional hygiene (NZ hygienist network), nightly night-guard use, radiographic review at months 12 and 36, and a clear escalation pathway for any prosthetic event in between. The maintenance contract is not separate from the treatment, it is the final phase of the treatment.
Curious about costs and timelines?
Common Mistakes
What are the most common mistakes patients make with full mouth rehabilitation?
> The three most common are: choosing a clinic based on price alone without verifying the diagnostic framework; skipping or shortening the provisional phase; and selecting a treatment plan before receiving a CBCT and full clinical assessment. A fourth, specific to international patients: failing to build a proper NZ hygienist relationship for the maintenance phase.
The most consequential mistakes in FMR happen before the first appointment, not during surgery. Choosing a clinic on the basis of the lowest quote, without verifying the diagnostic framework, the implant brand, the articulator workflow, or the written warranty, is the most common and most serious error. An FMR at 40% of the correct price typically means a 40% diagnostic phase, a 40% provisional phase, and the full clinical risk.
At Stunning Dentistry, the mistakes above have been catalogued across every patient interaction where an outcome was less than optimal. Every one of them was preventable at the planning stage. The pre-treatment checklists, the consent framework, the twelve consultation questions, they exist because the mistakes are predictable, and predictable mistakes can be engineered out.
Want a personalised treatment plan?

Myth Deconstruction
What are the most common myths about full mouth rehabilitation?
> Myth 1: FMR can be completed in one visit. False, a minimum 6-week provisional phase is non-negotiable for any well-planned FMR. Myth 2: Cheaper clinics use the same materials. False, material and implant system choice directly determines 10-year survival. Myth 3: FMR is only for extreme cases. False, moderate systemic wear with CR-MIP discrepancy qualifies. Myth 4: Dental tourism is always risky. False, risk is determined by clinical governance, not geography.
Full mouth rehabilitation can be done in one trip or one week.**
No. A minimum 6-week provisional phase, concurrent with implant osseointegration (3–6 months for implant-supported cases), is the non-negotiable biological and occlusal verification requirement for any properly planned FMR. Claims of "one-week full mouth" describe immediate-loading provisionals without a proper provisional phase, not an FMR. The provisional phase is not a logistical inconvenience; it is the diagnostic instrument that verifies the new bite before it is committed in permanent materials.
All clinics offering FMR use the same materials.**
Material choice directly determines 10-year survival. The difference between 3Y monolithic zirconia (400 MPa flexural strength; 10-year survival 94–97%) and feldspathic porcelain (60–80 MPa; 10-year survival 50–65% in reconstruction contexts) is not cosmetic. Similarly, the implant brand, Straumann, Nobel Biocare, Osstem, and the tier of that brand's implant system determine the long-term evidence base behind your fixtures. Asking for the brand name and the specific system is not pedantry; it is a clinical right.
FMR is only for the most extreme dental presentations.**
FMR is indicated whenever the dentition has reached the threshold where individual-tooth work can no longer restore function, this includes moderate systemic wear with VDO loss, patients with moderate-to-severe CR-MIP discrepancy, and patients whose multiple independent restorative episodes have been planned without a unified occlusal scheme. The case for FMR is not always visible in a mirror; it is visible on an articulator mounting.
Travelling to India for dental treatment is always risky.**
Risk is determined by clinical governance, implant system, material standard, and warranty structure, not geography. A New Zealand prosthodontist treating under a well-resourced protocol with Straumann fixtures, a proper articulator workflow, and a written lifetime warranty carries less clinical risk than an offshore clinic with unlisted implants and a verbal promise. The twelve consultation questions in this article are designed to assess risk directly, regardless of where the clinic is located.
Questions about this procedure?

People Also Ask
How long does full mouth rehabilitation take?
Monolithic zirconia (3Y, 4Y TZP) for posterior and high-load sites. Lithium disilicate (e.max) for anterior aesthetics. PMMA for provisionals. Straumann, Nobel Biocare, or Osstem implant systems.
Ready to discuss your options?
Ask Your Doctor
Bring these questions to any FMR consultation, at Stunning Dentistry, a New Zealand specialist, or anywhere else. A clinician who welcomes them is a clinician you can trust with a 9–18-month reconstruction.
1. Which diagnostic framework will govern my case, Dawson, Kois, Pankey, Hobo-Takayama, and why that one for my specific presentation?
2. Will the case be mounted on a semi-adjustable articulator with facebow transfer? Which articulator? What are the condylar inclination and Bennett angle settings?
3. What is my current VDO, and what will the new VDO be? Can I see both measurements in writing before I commit?
4. How long will the provisional phase be, and what will I be testing during it, VDO, CR, aesthetics, phonetics?
5. Who is on my clinical team, lead prosthodontist, implantologist, periodontist, orthodontist, and what is each person accountable for?
6. What implant system will you use and what prosthetic materials, brand, class, and 10-year survival data for each?
7. Can I see my CBCT, my digital wax-up, and the planned mock-up before anything irreversible happens?
8. What is the written warranty, on implants, prosthetic components, and labour, and what does it exclude?
9. What is your complication rate, and what is your revision protocol for screw loosening, crown chipping, and peri-implantitis?
10. How will I be followed up if I am in New Zealand and you are in India, specific protocol, not a general promise?
11. What is the 10-year maintenance cost projection, annual reviews, hygiene, night-guard replacement, component repair?
12. What happens if I have a prosthetic emergency in New Zealand three years after treatment, who do I call, what happens, and what does it cost me?
*Print this section. Bring it to your consultation. If any question is deflected, you have learned something important.*
Curious about costs and timelines?

Want a personalised treatment plan?
Book a Consultation
If you are uncertain whether full mouth rehabilitation is the right treatment, or whether the India pathway makes sense for your case, request a diagnostic evaluation.
Diagnosis precedes decision.
Questions about this procedure?

Ready to discuss your options?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Can FMR restore a bite worn down over twenty years?
Yes, where VDO can be re-established in provisional form and the patient adapts. Abduo's 2012 systematic review confirms adaptation to VDO increases up to 5 mm when tested in provisional form. Most patients with long-term wear adapt within 2–4 weeks of the new VDO.
Can FMR treat TMJ problems?
Sometimes. Where TMD is driven by occlusal instability (CR-MIP slide, VDO collapse, anterior guidance failure), FMR can resolve the symptoms. Where TMD is driven by internal derangement (disc displacement, joint degeneration), FMR treats the occlusal component only, joint pathology requires separate management.
Can I have FMR if I have untreated gum disease?
Not directly. Periodontal disease must be stabilised first, scaling, root planing, sometimes surgical periodontics, before restorative work begins. The pre-restorative periodontal phase is 3–6 months in most cases.
What if I change my mind halfway through?
FMR is sequenced to maximise reversibility until the definitive phase. The provisional phase is adjustable and extendable. If the patient does not approve the provisional design, it is revised rather than committed. The point of no return is cementation or screw retention of the definitive, everything before that is adjustable.
Will FMR affect my speech?
Temporarily. Speech adaptation to new anterior tooth positions typically takes 2–4 weeks during the provisional phase and resolves before the definitive is seated. Patients who have had missing anterior teeth for years often report improved speech post-FMR.
How long will the FMR last?
Designed for 10–15 years as a system, with expected minor maintenance. Published 10-year survival for fixed implant-supported prostheses is 89–95%; for tooth-supported crowns and bridges in rehabilitation contexts, 85–92%. With night-guard compliance and structured maintenance, individual cases routinely exceed the median.
What is the warranty on the FMR at Stunning Dentistry?
Lifetime warranty on implants. Documented warranty period on prosthetic components. Written warranty document issued at definitive delivery. Repair and replacement within warranty terms carries no additional surgical fee.
How is my case handled between India visits?
Bi-weekly Zoom check-ins with the assigned prosthodontist for the first 8 weeks. Monthly Zoom reviews thereafter. NZ hygienist visit at month 3 (referral letter provided). 24/7 CRM access, response within 4 business hours, 24 hours overnight. Photo and radiograph upload to the clinical portal.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










